Truncus arteriosus is a rare congenital heart defect that affects how blood flows out of your baby’s heart. Instead of a separate pulmonary artery and aorta, your baby has a single vessel called a truncus. This interferes with normal blood flow to your baby’s lungs and the rest of their body. Surgery within weeks of birth can be lifesaving.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
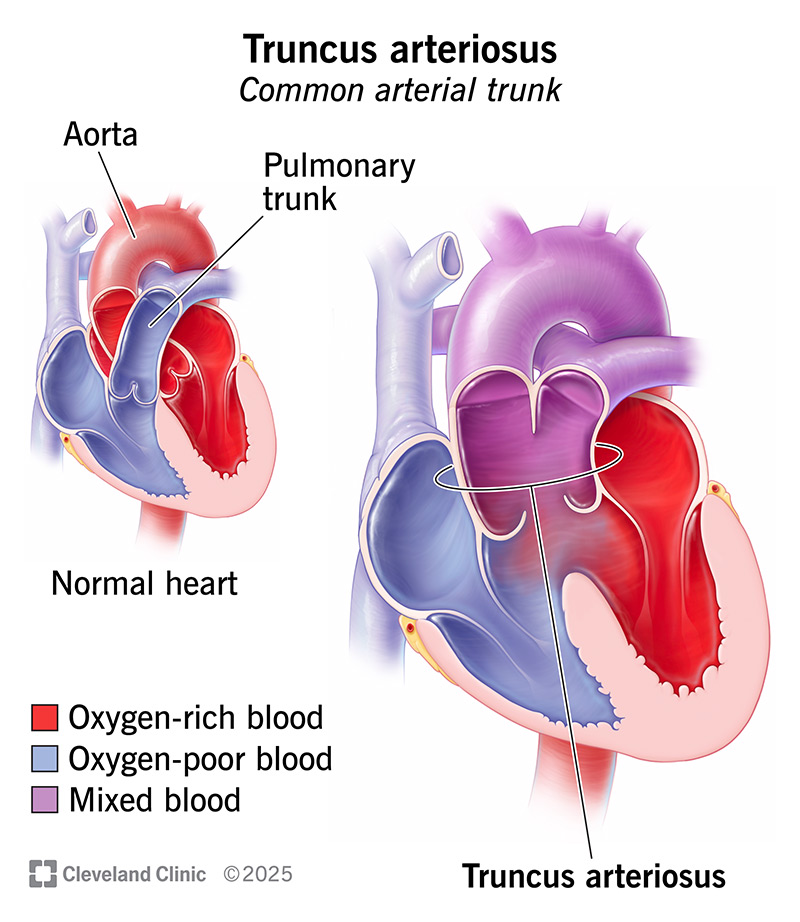
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/14785-truncus-arteriosus)
Truncus arteriosus is a rare heart defect that some babies are born with. It means there’s just one artery that carries blood out of your baby’s heart, rather than two. Normally, the aorta sends oxygen-rich blood to the body. And the main pulmonary artery sends oxygen-poor blood to the lungs.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
But with truncus arteriosus, these two arteries are combined as a single vessel that sends mixed blood to your baby’s lungs and their body.
Truncus arteriosus overworks your baby’s heart and lungs. It makes their heart pump too much blood to their lungs. It also prevents their organs and tissues from receiving enough oxygen. That’s why healthcare providers call it a critical congenital heart defect. Babies need treatment right away to survive.
Your baby will likely have surgery within weeks of birth. Surgeons can create two separate paths for blood to flow out of your baby’s heart. This reduces the strain on their heart and lungs and lets their body get enough oxygen. As your child grows and the oxygen needs for their organs change, they’ll need more surgeries to keep their heart working as it should. Their care team will be with you each step of the way.
Signs and symptoms typically appear within the first few days of life. You might notice some on your own. Healthcare providers may notice others during a check-up. Newborns with truncus arteriosus may have:
Advertisement
About 1 in 3 babies with truncus arteriosus have DiGeorge syndrome. This is a genetic disorder that may cause signs and symptoms affecting other parts of their body, too.
Truncus arteriosus happens when the fetal heart doesn’t develop as it should during pregnancy. In most cases, there’s no clear reason why. But if your child has DiGeorge syndrome, the gene changes that cause the disorder are responsible for this heart defect.
Normally, a fetal blood vessel called the truncus separates into two distinct arteries before your baby is born. A wall of tissue called the aortopulmonary septum marks the boundary between the two vessels and prevents blood from mixing.
But for unknown reasons, the truncus might not form in this way. Instead, the truncus remains (persists) as a single common artery. That’s why healthcare providers sometimes call this condition “persistent truncus arteriosus” or “common arterial trunk." The truncus itself is a normal part of fetal development. But it’s not supposed to persist past birth.
Your baby may have a higher risk of developing truncus arteriosus or other forms of congenital heart disease if you’re pregnant and:
Healthcare providers usually diagnose truncus arteriosus during your baby’s first few days of life when symptoms appear. If providers suspect a heart issue, they perform an echocardiogram. This test can show truncus arteriosus and other heart issues.
It’s also possible for pulse oximetry — part of routine newborn screenings — to show low oxygen levels before other signs develop.
Sometimes, providers notice truncus arteriosus before birth on a prenatal ultrasound. If your provider thinks there might be a heart defect, they may do a fetal echocardiogram. This test shows fetal heart anatomy in more detail.
Your child’s care team may mention a specific type of truncus arteriosus. These types describe the anatomy of your child’s left and right pulmonary arteries, which carry blood to their lungs. These arteries normally branch off the main pulmonary artery. But with truncus arteriosus, the branch arteries start in different spots:
Advertisement
Other variations are possible. Healthcare providers use this knowledge of your child’s anatomy to guide surgery.
Babies with truncus arteriosus usually also have both of the following:
Other heart defects that may occur with truncus arteriosus include:
Babies with truncus arteriosus need heart surgery within the first weeks of life. The most common procedure is called a Rastelli repair. This creates two separate paths for blood to leave your baby’s heart.
Advertisement
Your baby’s surgeon will:
These are the basic steps for truncus arteriosus repair. Your baby’s surgery may include other steps if they have other heart defects that need repair. Their surgeon will explain exactly what’s needed for their unique heart anatomy.
Down the road, your child will need more surgeries to keep their heart and blood vessels working normally. For example, the artificial pulmonary conduit doesn’t grow with your child. So, they’ll need a new one that’s typically larger in size as they get older. Your child may also have issues with their heart valves.
Your child’s surgeon will tell you more about future surgeries and what they’ll involve. Your child will likely need another surgery within three to 10 years after their first one, and possibly more after that.
Seek medical care right away if your baby doesn’t seem well in their first few days of life. Some truncus arteriosus signs, like bluish skin tone and trouble feeding, can also point to other serious heart issues.
Advertisement
Follow-up care is very important after truncus arteriosus repair. Your baby’s care team will explain what’s needed and when.
Over the years, you’ll work closely with a heart specialist called a pediatric cardiologist. They’ll run tests to monitor your child’s heart and plan the best timing for other treatments or surgeries.
How long children with truncus arteriosus live depends on many things, including the complexity of their heart anatomy and other health conditions they have. In general, research shows:
Numbers don’t always tell the full story. Your child’s care team can give you the best sense of what to expect and how to support your child.
If you’ve just learned your baby has truncus arteriosus, you might feel scared or overwhelmed. You may want to learn every possible thing about this diagnosis and what it could mean for your baby’s future. Understanding the science is important. But also keep in mind that heart issues affect each baby a little differently.
Lean on your child’s care team for insight and guidance. It may also help to connect with an organization that supports families of children with congenital heart disease. Learning from other parents with similar experiences can help you feel supported and understood.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When you need heart surgery, you want the most experienced team on your side. Cleveland Clinic offers expert cardiology care and heart surgery.
