Fecal incontinence, also called bowel incontinence, happens when you have trouble managing or controlling when you have a bowel movement (poop). Stool (feces/waste) leaks out without your control. Depending on the cause, treatment can include dietary changes, exercises, medications or surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
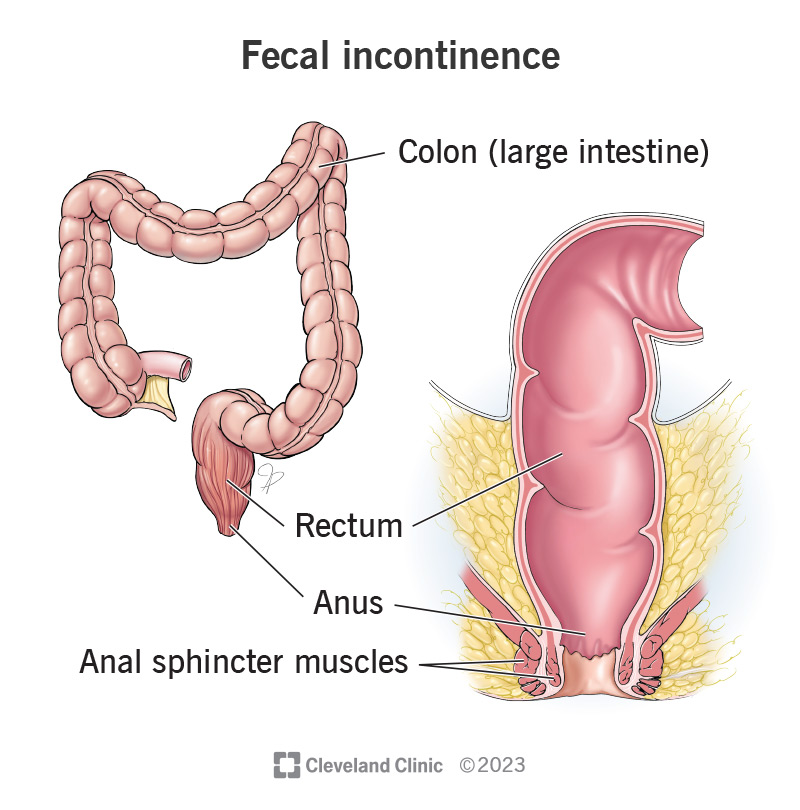
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/Images/org/health/articles/14574-fecal-bowel-incontinence.jpg)
Fecal incontinence — also called bowel incontinence — is when you can’t manage or control your bowel movements (pooping). Liquid or solid stool (poop) leaks out when you don’t want it to. Fecal incontinence may be as mild as having a little leakage when you pass gas or as severe as unintentionally passing solid stools.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Several factors affect your ability to regulate bowel movements. The muscles in your pelvic floor, rectum and anus must be working correctly to hold poop and (when the time’s right) release it. Nerves have to work with these muscles so your body knows when it’s time to poop. Finally, you have to be physically able to reach the toilet in time.
If any of these things go awry, you may have issues with fecal incontinence.
There are two types of fecal incontinence:
It’s very common. Researchers estimate that it affects 1 in 3 people — or even more. Bathroom visits are a private matter; many people have likely experienced fecal incontinence at some point or another but just don’t talk about it.
Advertisement
Some people only have issues with leakage when they have diarrhea (runny stools). For others, fecal incontinence is an ongoing experience. Signs and symptoms include:
The most common causes of fecal incontinence include constipation, diarrhea and conditions that damage the muscles or nerves that help you poop. Prior surgeries and procedures can also play a role.
Anyone can experience fecal incontinence, but your risk is greater depending on your:
Conditions that cause muscle or nerve damage or tissue scarring can increase your risk of fecal incontinence, including:
The leakage can take a toll on your skin around your butthole (anus), causing it to feel irritated. This can include the feeling of burning, itching, and throbbing pain. Eventually, you may develop sores (ulcers). You can take steps to care for your skin to prevent this from happening.
But not all complications are physical. A greater concern for most people with fecal incontinence is the toll it can take on your mental and emotional well-being. It’s common to feel embarrassed, anxious or stressed over the leakage. It can prevent you from being as social as you’d like. It’s essential to seek care and support so the condition doesn’t cause you to isolate or compromise your mental health.
Advertisement
You’ll see a gastroenterologist or a colorectal surgeon, specialists trained to help you. Your healthcare provider will ask you questions about your symptoms and do a physical exam and a rectal exam. Don’t be embarrassed to talk freely about the issues you’re having.
You may need the following tests to find what’s causing the leakage:
Advertisement
You may need a blood test or stool test to check for causes of frequent diarrhea, like infection-causing microbes (bacteria, viruses and parasites).
Depending on what’s causing your fecal incontinence and how severe it is, you may need surgery, therapy or medications. In some instances, you can manage fecal incontinence with lifestyle changes.
You can change what you eat and drink to manage incontinence related to diarrhea or constipation. It’s a good idea to track what you consume daily, noting what foods or drinks make you less likely to have healthy bowel movements. Then, do everything you can to avoid them.
For diarrhea, avoid foods that can loosen your stools or make you have to go, including:
For constipation, change your eating and drinking habits to prevent chronic constipation. This includes:
Exercises and training condition your body to maintain better control over your bowel movements. Some types you can do at home. Others you do in a provider’s office or under the guidance of a trained therapist.
Advertisement
Medications include anti-diarrheal drugs and medicines that treat constipation, like bulk laxatives, suppositories or enemas. Don’t use over-the-counter (OTC) medications without checking with your healthcare provider first. If an OTC medicine isn’t doing the trick, you may need a prescription medicine to manage the leakage.
Medicines for diarrhea include:
Medicines for constipation (and occasionally diarrhea) include:
Your experience depends on what’s causing your fecal incontinence and how treatable it is. For example, if fecal incontinence is related to an infection (as with diarrhea), relief may be as straightforward as a round of antibiotics to kill the bacteria.
Therapies like biofeedback help many people improve their bowel control, but much depends on the nature of your condition before you start treatment.
Treatments for fecal incontinence, including surgery and sacral stimulation, improve fecal incontinence for some people but not for others. Research shows symptoms improve for over half of people following sphincteroplasty or sacral stimulation. However, over time, symptoms may gradually return for some people. If you need surgery for fecal incontinence, you’ll typically also need long-term symptom management.
You can’t prevent all causes of fecal incontinence. But you can take steps to lower your risk of two of the most common ones: diarrhea and constipation.
Don’t delay seeking treatment if you have diarrhea. Incorporate changes to your diet that reduce your risk of constipation. And if you’re constipated, don’t strain to poop. This can damage the nerves and muscles that help you control bowel movements.
You can take steps to protect your physical and emotional well-being if you’re living with fecal incontinence.
Fecal leakage can irritate your skin and lead to excess moisture or sores. To protect your skin:
Caring for your mental health (and prioritizing your social life) is as important as caring for your physical health. To cope:
From the time we were little, many of us learned it was bad manners to talk about poop or bathroom visits. Many people carry this mindset into adulthood — and feel ashamed of issues like incontinence. But the truth is, pooping is a normal part of your (and everyone else’s) health. And sometimes, maintaining good health requires discussing what’s going wrong with your provider. Don’t be ashamed to discuss your symptoms with your healthcare provider. They can recommend treatments and strategies that can help you regain better control over your bowel movements.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s experts can treat fecal incontinence with the help of therapies, including dietary changes, pelvic floor exercises, medication and surgery.
