Uterine cancer includes two types of cancer: endometrial cancer (more common) and uterine sarcoma (rare). Uterine cancer symptoms include bleeding between periods or after menopause. Treatment often consists of a hysterectomy to remove your uterus.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
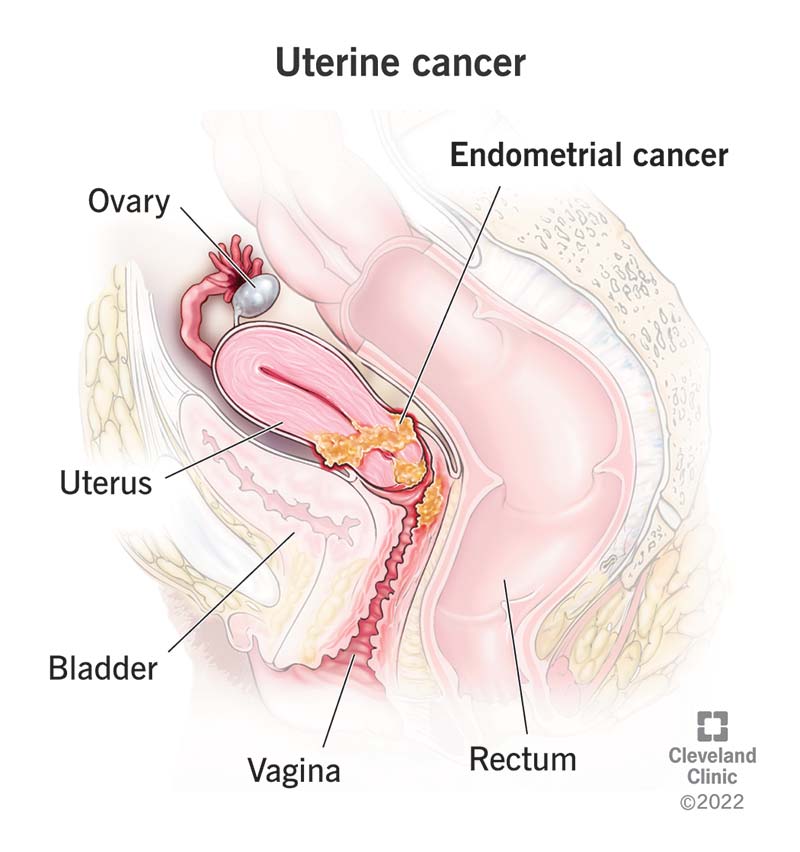
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/16409-uterine-endometrial-cancer)
Uterine cancer is a general term that describes cancer in your uterus:
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Uterine cancer can refer to either endometrial cancer or uterine sarcoma. But people often consider the terms “endometrial cancer” and “uterine cancer” the same. That’s because endometrial cancer makes up about 95% of all cases of uterine cancer. A diagnosis of uterine sarcoma is rare.
The uterus is part of the reproductive system of women. It’s where a fetus develops during pregnancy.
The top part of your uterus is called the body or corpus. At the end of your uterus is your cervix, which connects your uterus to your vagina. Uterine cancer refers to cancer in the body of your uterus. Cancer in your cervix — cervical cancer — is a different type of cancer.
The endometrium is the inner layer of your uterus. It changes during your menstrual cycle.
Hormones called estrogen and progesterone cause the endometrium to thicken in case of pregnancy. If no pregnancy occurs, your body produces less progesterone which causes the endometrial lining to shed. That’s when periods take place.
Advertisement
In the United States, endometrial cancer is the most common cancer affecting the reproductive system of women. Endometrial cancer mainly develops after menopause. About 3% of women will receive a diagnosis of uterine cancer at some point during their lives. Each year, about 65,000 women receive a diagnosis.
Video content: This video is available to watch online.
View video online (https://cdnapisec.kaltura.com/p/2207941/sp/220794100/playManifest/entryId/1_js847sjb/flavorId/1_5f3sgelj/format/url/protocol/https/a.mp4)
Risk factors for uterine cancer.
Signs of uterine cancer can resemble those of many conditions. That’s especially true of other conditions affecting reproductive organs. If you notice unusual pain or irregular vaginal bleeding, talk to your healthcare provider. An accurate diagnosis is important so you can get the proper treatment.
Symptoms of endometrial cancer or uterine sarcoma include:
Researchers aren’t sure of the exact cause of uterine cancer. Something happens to create changes in cells in your uterus. The mutated cells grow and multiply out of control, which can form a mass called a tumor.
Certain risk factors can increase the chances you’ll develop uterine cancer. If you’re at high risk, talk to your healthcare provider about steps you can take to protect your health.
There are several risk factors for endometrial cancer. Many of them relate to the balance between estrogen and progesterone. These risk factors include having obesity, a condition called polycystic ovarian syndrome (PCOS) or taking unopposed estrogen (taking estrogen without taking progesterone, too). The genetic disorder Lynch syndrome is another risk factor unrelated to hormones.
Risk factors include:
Advertisement
The most serious complication of endometrial cancer is death. However, when your healthcare provider diagnoses endometrial cancer at an early stage, the prognosis is usually very good.
Advertisement
Other complications of endometrial cancer include:
Talk to your healthcare provider if you notice possible signs of uterine cancer. Your provider will:
Your provider may perform one or more tests to confirm a diagnosis of uterine cancer:
Blood tests:
Imaging tests:
Other tests:
Advertisement
If you had a D&C or biopsy to remove tissue samples, your provider then sends the sample to a lab. There, a pathologist looks at the tissue to confirm if there’s cancer.
No. The Pap test (Pap smear) doesn’t screen for or diagnose uterine cancer. It checks for cervical cancer.
If your healthcare provider diagnoses endometrial cancer, they also need to determine the type. Knowing the cancer type helps your care team figure out the best treatment:
Your provider will also determine cancer stage. Uterine cancers are staged on a scale that ranges from I to IV.
In some cases, your provider may not be able to determine what stage of cancer you have until you’ve had surgery to remove it.
Most women with endometrial cancer need surgery. Your particular treatment plan depends on the type of cancer and your overall health. Other treatments you may have include:
Researchers continue to study more ways to treat endometrial cancer.
Surgery is usually the primary treatment for endometrial cancer. You’ll most likely have a hysterectomy, with the surgeon removing your uterus and cervix. There are four types of hysterectomy procedures:
During a hysterectomy, surgeons often perform two other procedures, as well:
Many women who have uterine cancer need their ovaries removed. But removing the ovaries means you’ll go through menopause if you haven’t already. If you’re younger than 45 and premenopausal, talk to your care team to see if you should keep your ovaries.
Side effects of uterine cancer surgery include:
Often, surgeons use a single procedure to diagnose, stage (describe severity) and treat uterine sarcoma. Treatment options are like those for endometrial cancer. You may have a hysterectomy, as well as a BSO to remove your ovaries and fallopian tubes.
The five-year survival rate for endometrial cancer is 81%. That means 81% of women diagnosed with the disease are alive five years later. The rate is even higher when cancer hasn’t spread outside your uterus. Then, the survival rate reaches as high as 95%. Treatments continue to improve, along with survival rates. Uterine cancer is fatal when it goes undiagnosed and spreads. The survival rate decreases to 17% when cancer spreads to other parts of your body outside your uterus. Early detection and early treatment are key to a favorable prognosis.
Fortunately, endometrial cancer is often diagnosed at an early stage. That’s because many people notice unusual bleeding and tell their healthcare providers. If cancer gets caught early and hasn’t spread to other organs, removing your uterus can cure it.
Most of the time, you can’t prevent uterine cancer. But you can take steps to reduce your risk by:
If you’re considering ERT, talk to your healthcare provider. Together, you can discuss your cancer risk and make the decision that’s best for you.
No, there’s no screening tool. And healthcare providers usually don’t recommend regular testing for people without symptoms. They may do so if you’re at higher risk, though. If you’re at high risk, talk to your provider about regular checks for uterine cancer.
Discuss any unusual bleeding or spotting with a provider. If you have an inherited endometrial cancer risk (passed down through genes), talk to your provider about yearly testing. You may need an endometrial biopsy every year, starting at age 35.
If you’ve received a uterine cancer diagnosis, ask your provider:
After you finish treatment, your care team will talk to you about your follow-up visits. It’s important to go to these appointments. During a follow-up visit, your provider will do a pelvic exam. They’ll also ask you about any symptoms. The goal is to make sure cancer isn’t coming back (recurring) and that you’re feeling OK after treatment.
You can also talk to your provider about ways to live a healthy life after cancer. Eating well, getting enough sleep and exercising can help you feel your best.
Let your provider know about any irregular bleeding. Abnormal bleeding includes bleeding between periods if you still menstruate and bleeding or spotting if you’re postmenopausal. Abnormal bleeding is a symptom of many conditions, including endometrial cancer.
Type 1 cancers, the most common type, don’t spread quickly. Type 2 cancers can spread quickly and may require more aggressive treatment.
Endometrial cancer is most common in people who’ve gone through menopause. The average age of menopause is 51.
Uterine cancer includes endometrial cancer and uterine sarcoma. It’s the most common cancer affecting women's reproductive systems. Often, healthcare providers use the term endometrial cancer to describe uterine cancer because it’s the most common. Uterine cancer symptoms include vaginal bleeding between periods or after menopause. If healthcare providers catch uterine cancer before it spreads, surgery can cure it. If you experience any signs of uterine cancer, contact your healthcare provider.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When you have endometrial cancer, you’ll want the best care. Cleveland Clinic’s experts are here to help with personalized treatment focusing on your needs.
