Gallstones (cholelithiasis) are hardened pieces of bile that form in your gallbladder or bile ducts. They’re common, especially in females. Gallstones don’t always cause problems, but they can if they get stuck in your biliary tract and block your bile flow. If your gallstones cause you symptoms, you’ll need treatment to remove them — typically, surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
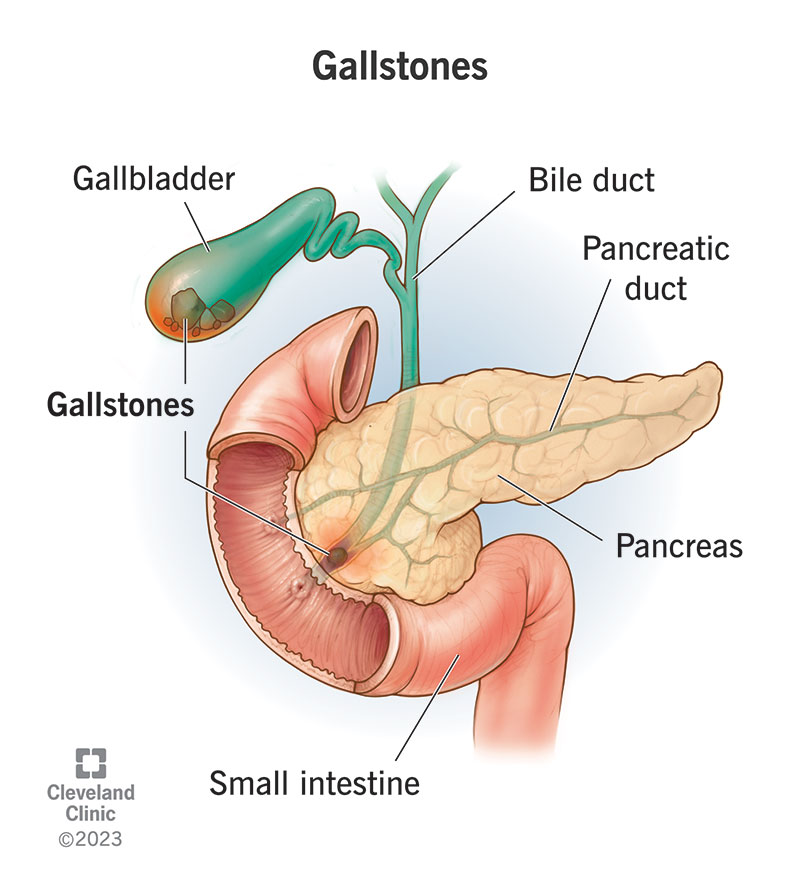
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/Images/org/health/articles/7313-gallstones.jpg)
Gallstones are hardened, concentrated pieces of bile that form in your gallbladder or bile ducts. “Gall” means bile, so gallstones are bile stones. Your gallbladder is your bile bladder. It holds and stores bile for later use. Your liver makes bile, and your bile ducts carry it to the different organs in your biliary tract.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Healthcare providers sometimes use the term “cholelithiasis” to describe the condition of having gallstones. “Chole” also means bile, and “lithiasis” means stones forming. Gallstones form when bile sediment collects and crystallizes. Often, the sediment is an excess of one of the main ingredients in bile.
Gallstones (cholelithiasis) won’t necessarily cause any problems for you. A lot of people have them and never know it. But gallstones can become dangerous if they start to travel through your biliary tract and get stuck somewhere. They can clog up your biliary tract, causing pain and serious complications.
The problem with gallstones is that they grow — slowly, but surely — as bile continues to wash over them and leave another layer of sediment. What begins as a grain of sand can grow big enough to stop the flow of bile, especially if it gets into a narrow space, like a bile duct or the neck of your gallbladder.
At least 10% of U.S. adults have gallstones, and up to 75% of them are female. But only 20% of those diagnosed will ever have symptoms or need treatment for gallstones.
Video content: This video is available to watch online.
View video online (https://cdnapisec.kaltura.com/p/2207941/sp/220794100/playManifest/entryId/1_ikvpu2v4/flavorId/1_5f3sgelj/format/url/protocol/https/a.mp4)
Christine Lee, MD, explains what gallstones are and how they’re treated.
Gallstones generally don’t cause symptoms unless they get stuck and create a blockage. This blockage causes symptoms, most commonly upper abdominal pain and nausea. These may come and go, or they may come and stay. You might develop other symptoms if the blockage is severe or lasts a long time, like:
Advertisement
Typical gallstone pain is sudden and severe and may make you sick to your stomach. This is called a gallstone attack or gallbladder attack. You might feel it most severely after eating, when your gallbladder contracts, creating more pressure in your biliary system. It might wake you from sleep.
Gallstone pain that builds to a peak and then slowly fades is called biliary colic. It comes in episodes that may last minutes to hours. The episode ends when and if the stone moves or the pressure eases. People describe the pain as intense, sharp, stabbing, cramping or squeezing. You might be unable to sit still.
Your biliary system is located in the upper right quadrant of your abdomen, which is under your right ribcage. Most people feel gallstone pain in this region. But sometimes, it can radiate to other areas. Some people feel it in their right arm or shoulder or in their back between their shoulder blades.
Some people feel gallstone pain in the middle of their abdomen or chest. This can be confusing because the feeling might resemble other conditions. Some people mistake gallstone pain for heartburn or indigestion. Others might feel like they’re having a heart attack, which is a different emergency.
No, but females may be more likely to experience referred pain — pain that you feel in a different place from where it started. So, they may be more likely to experience gallstone pain in their arm, shoulder, chest or back.
Females are also more prone to chronic pain, and they may be more likely to dismiss pain that comes and goes, like biliary colic does. It’s important to see a healthcare provider about any severe or recurring pain, even if it goes away. Once you’ve had a gallstone attack, you’re likely to have another.
Gallstone pain means that a gallstone has gotten stuck in your biliary tract and caused a blockage. If it’s a major blockage, you might feel it right away. If it’s only a partial blockage, you might not notice until your gallbladder contracts, creating more pressure in your system. Eating triggers this contraction.
A rich, heavy or fatty meal will trigger a bigger gallbladder contraction. That’s because your small intestine detects the fat content in your meal and tells your gallbladder how much bile it will need to help break it down. Your gallbladder responds by squeezing the needed bile out into your bile ducts.
Biliary colic is the only warning sign of gallstones that you’ll get. It happens when a gallstone causes a temporary blockage, then manages to move out of the way and let bile flow through again. Even though the pain eventually goes away, it’s important to recognize these episodes as the warning that they are.
Advertisement
Once a gallstone has caused a blockage in your biliary tract, it’s likely to keep happening. The same one may be hanging around the same tight spot and continuing to grow. Or you may have more gallstones waiting in the wings. One day, a gallstone might get stuck and stay stuck. This would be an emergency.
If a gallstone blocks the flow of bile through your biliary system, it can affect any or all of the organs in that system. Bile that can’t flow backs up into your bile ducts and organs, causing acute inflammation and encouraging bacterial infections. When severe, these conditions can become life-threatening.
Complications include:
Dizziness and fatigue are symptoms of low blood pressure. These aren’t typical symptoms of gallstones. However, low blood pressure is a possible side effect of gallstone complications. Severe inflammation or infection in your biliary system could trigger a faster heart rate along with a drop in blood pressure.
Gallstones form when there’s an excess of one of the main ingredients in bile. The excess ingredient turns to sediment at the bottom of your gallbladder or bile ducts, and the sediment gradually hardens into stones. Cholesterol stones are the most common type. Pigment (bilirubin) stones are the other.
Advertisement
A variety of factors may be involved in this process, including:
Advertisement
A variety of diseases and conditions can affect your bile flow or your cholesterol, bilirubin or bile acid levels. But not everyone with gallstones has an underlying condition. Some of the most common risk factors are normal factors, like your age, genetic profile, hormone levels and weight fluctuations.
Risk factors include:
If you’re experiencing gallstone symptoms, your healthcare provider will investigate with blood tests and imaging tests. Blood tests can detect inflammation, infection or jaundice and offer clues to which organs are affected. Imaging tests will help locate the source of the blockage in your biliary tract.
Your provider will begin with an abdominal ultrasound, which is a quick and easy test that doesn’t require any preparation. An ultrasound can find most gallstones in and around your gallbladder. But if a gallstone is stuck somewhere else in your biliary tract, you may need another kind of test to find it.
Other possible tests include:
If your gallstones never cause problems, you won’t need treatment for them. But if gallstones cause a blockage in your biliary tract, your healthcare provider will want to remove them — not just the blockage, but all of them. Once gallstones have caused a blockage, they’re highly likely to do so again.
Most people who need treatment for gallstones will have surgery to remove them. Surgery is the only way to ensure gallstones won’t cause issues for you again. But if you can’t or don’t want to have surgery, there are some alternative treatments to try, including medications and other procedures.
Gallbladder removal (cholecystectomy) is the only reliable long-term solution for gallstones. It’s one of the most common procedures performed worldwide, usually as a laparoscopic surgery. You can live well without a gallbladder. From now on, bile will simply flow directly from your liver to your small intestine.
Occasionally, some people who need treatment for gallstones aren’t in a safe condition to have gallbladder removal surgery. In these cases, cholecystostomy is one alternative. This minor procedure places a catheter in your gallbladder to drain it. It can remove the gallstones currently inside.
Healthcare providers don’t prescribe medications for gallstones very often because they aren’t very effective. Medications like ursidol and chenodiol only work on smaller cholesterol stones that haven’t caused any complications yet. It can take months to years to dissolve them, and they often return.
This isn’t a practical way to treat gallstones for most people. But there may be limited circumstances where medications are helpful as a temporary or preventive measure. If you’re not a good candidate for gallstone surgery, your healthcare provider will discuss their recommendations with you.
After surgery, most people will never need treatment for gallstones again. Complications are uncommon, but some people develop chronic diarrhea. This is because bile now flows continuously to your intestines, instead of on demand. You can treat it with medications called bile acid binders.
There’s no sure way to prevent gallstones from forming, but you can take certain steps to reduce your overall risk. For example, you can reduce your risk of cholesterol stones, which are by far the most common type, by reducing cholesterol in your diet. However, this won’t prevent pigment stones.
If you have overweight or have obesity, losing some weight can reduce your risk of cholesterol stones. But losing weight fast can raise your risk. If you’re expecting rapid weight loss from a procedure or other treatment, your healthcare provider might recommend taking gallstone medications preventatively.
Gallstones won’t go away without treatment. Gallstones can sometimes come out in your poop, but it won’t be all of them. Even if your provider removes a gallstone from your bile duct, there will be others left behind, and you can get new ones. Gallbladder removal is the only way to make them stop for good.
A gallstone that makes its way into your common bile duct may pass all the way through to your intestines if it doesn’t get stuck along the way. From your intestines, it can pass out in your poop. That’s a lucky scenario, but you can’t expect that outcome from every gallstone, and you can’t make it happen.
There’s no way to make your gallstones enter your common bile duct, and there’s no way to ensure they’ll pass safely through to your intestine. They might just hang around in the duct and continue to grow. In general, you don’t want to risk having gallstones in your common bile duct in the first place.
You probably won’t feel a gallstone passing out of you. For a gallstone to pass successfully through your common bile duct into your intestines, it needs to be less than 5 millimeters. This is too small for you to feel in your intestines, although you might feel pain briefly while it passes through your common bile duct.
A gallstone that’s small enough to pass through your common bile duct might be too small to notice in your poop, even if you’re looking for it. But if you saw a gallstone in the toilet, it would look like a tiny pebble. The shape might look angular rather than smooth. Most are yellow, but some are brown.
You can’t pass gallstones in your pee, because there’s no way for gallstones to get into your urinary tract. Stones in your urinary tract are kidney stones. Gallstones and kidney stones are similar, but they travel through different pipelines. Painful urination is a symptom of kidney stones, not gallstones.
If you develop sudden stabbing pain in your upper right abdomen or shoulder, especially after eating, you might be having a gallbladder attack. Seek medical attention right away. Don’t wait for it to go away because it might not. A healthcare provider can relieve your pain while confirming the cause.
If you think you’ve experienced biliary colic in the past, even if it’s over, see your provider. They’ll take images of your biliary system to look for gallstones. If they find them, they’ll recommend treating them before they can cause further problems. Without treatment, gallstones will continue to form and grow.
Gallstones are common, and most people will never be bothered by them. If they stay put, you may never know they’re there. But once they begin to move, they become dangerous. These tiny, pebble-like pieces can do a lot of damage when they get into tight spaces in your delicate biliary system.
A gallstone attack is an awful way to find out that you have gallstones. You might be even more alarmed to learn that the recommended treatment is surgery. But gallbladder removal is a common procedure with an excellent prognosis. Your whole ordeal could be over within hours of your first symptoms.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
If you have issues with your digestive system, you need a team of experts you can trust. Our gastroenterology specialists at Cleveland Clinic can help.
