Double outlet right ventricle (DORV) describes a heart with two major arteries linking to its right ventricle (heart chamber). Normally, only one of these arteries connects to each ventricle. The double link is a rare, congenital (since birth) heart issue. Surgery repairs the problem, but children born with DORV need lifelong follow-up care.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
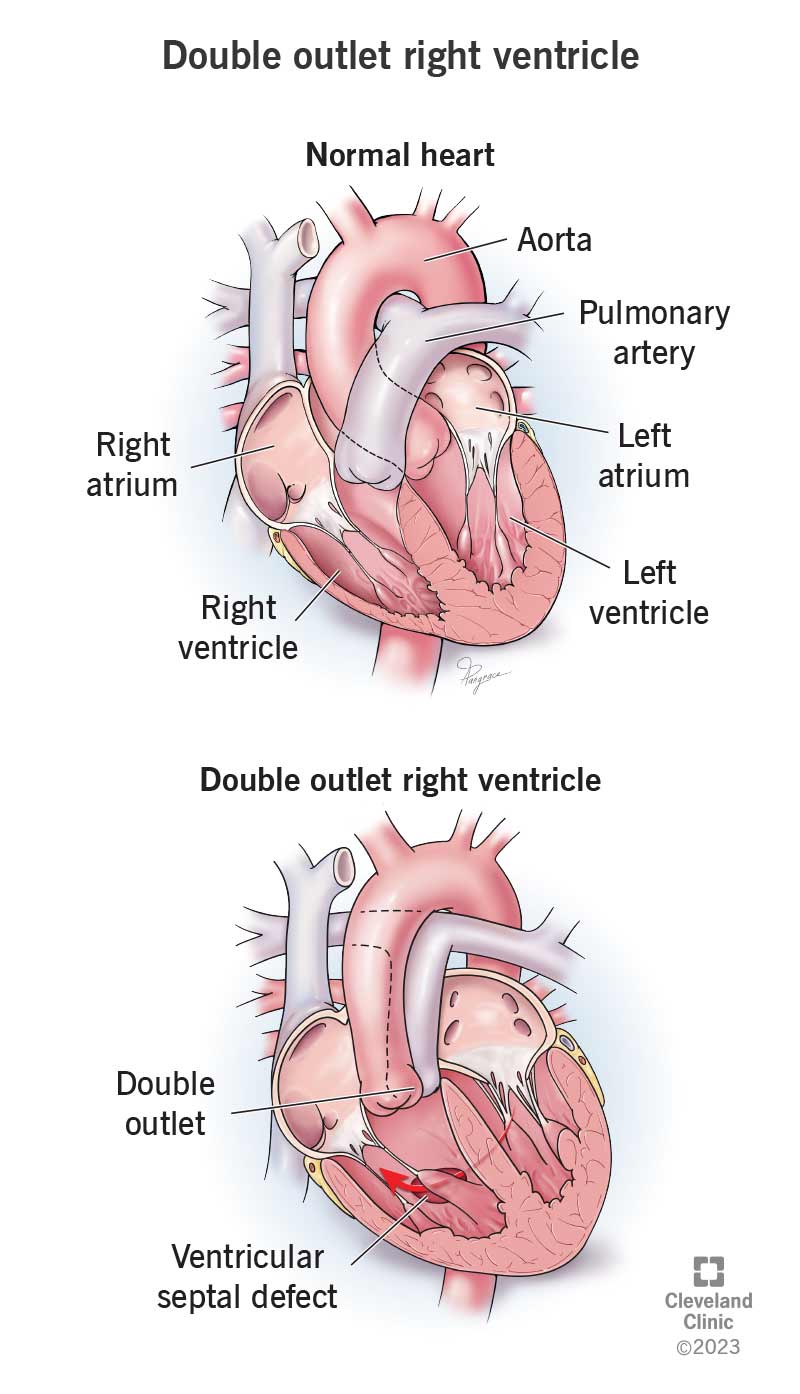
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/double-outlet-right-ventricle)
Double outlet right ventricle (DORV) is an abnormal heart issue in which your pulmonary artery and aorta connect to your right ventricle. In a typical heart, only one of them (pulmonary artery) connects there. This is a congenital heart condition, which means you’re born with it.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Usually, your pulmonary artery branches off from your right ventricle and your aorta branches off from your left ventricle. With DORV, your left ventricle connects to just a part of one of these arteries or no artery at all.
Double outlet right ventricle is a cyanotic heart disease. That means it can send blood without enough oxygen in it to your body. Also, your lungs may receive too much blood flow, which makes your heart work harder and can damage your heart and lungs.
DORV is rare. It happens in about 2 out of 10,000 newborns. Most will need surgery as infants.
Babies with a DORV heart defect often have other problems at birth, like:
Babies with double outlet right ventricle always have a ventricular septal defect (VSD), too. This hole in the septum, or wall between the two ventricles, lets blood flow between them.
Advertisement
Healthcare providers describe DORV types by the location of the VSD:
Double outlet right ventricle symptoms usually appear during the first days or weeks after birth. They include:
Researchers don’t completely understand what causes double outlet right ventricle. It’s a problem with fetal development. In half of cases, it happens to babies who have genetic syndromes.
Possible complications of a DORV heart defect include:
Sometimes, healthcare providers can find a heart defect like DORV before a baby is born. They may do this during a routine ultrasound screening called a fetal echocardiogram.
If not, a provider usually diagnoses double outlet right ventricle in the days or weeks after birth because of a baby’s symptoms.
During an exam, a provider will look for signs of low oxygen levels, like blue lips. They’ll use a stethoscope to listen to your baby’s heart. Another test they’ll use is pulse oximetry screening. This is a painless way to measure the amount of oxygen in your baby’s blood.
Your baby’s provider may order one or more tests, like:
Almost all babies with DORV need open-heart surgery within their first year of life. Your healthcare provider will help you make decisions about a double outlet right ventricle repair. They’ll consider your child’s overall health, the type of DORV heart defect they have, and other issues with your baby’s heart or other organs.
Advertisement
Your baby’s surgeon may take one of these approaches to double outlet right ventricle treatment:
Your provider will tell you how often your child will need checkups or more tests. It’s important to take your child to their follow-up visits to be sure they’re not developing any issues. Also, make sure your child is taking any medicines their provider prescribed.
Even after a surgical repair for double outlet right ventricle, your baby can have abnormal heart rhythms. They can develop heart failure years later, as well. Contact your provider if your child has an abnormal heart rhythm or signs of heart failure, like chest pain or shortness of breath.
Take your child to the emergency room if they’re having trouble breathing and/or their nails, lips or skin have a blue tint.
Advertisement
Questions to ask your provider may include:
Without surgery, a baby with double outlet right ventricle will develop high blood pressure in their lungs and heart failure.
With surgery, most babies who have this condition live to be adults. Anyone who’s had surgery for DORV needs lifelong care from a heart expert. Many children need another operation years later.
Because of the risk of infective endocarditis, some people with DORV need to take antibiotics before certain dental work. Taking care of your skin and teeth can also help prevent endocarditis.
People who had a surgical repair for DORV can carry a pregnancy. But providers don’t recommend it in certain situations. If you’re an adult who had an operation for this condition as a child, talk to your provider if you’re considering pregnancy.
With biventricular repair, people often live normal lives with at least an average lifespan. People who need other procedures may have shorter lifespans and need further surgery later in life. About 8 or 9 out of 10 people survive at least 10 years after surgery.
Advertisement
Finding out that your newborn has a heart issue is very upsetting, to say the least. But it’s not your fault. Researchers don’t know the cause. Focus on finding out what you can about your child’s needs so you can make informed decisions.
It can help to talk things over with a trusted friend or family member. Surgery and regular checkups can help people born with double outlet right ventricle live healthier, longer lives.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When your child has a heart problem, it’s natural to be anxious. Cleveland Clinic Children’s can diagnose and treat double outlet right ventricle.
