Overview
Cleveland Clinic began offering J-Pouch surgery in 1983. In 2002 it became the world's first Pouch Center.
- The Pouch Center now performs about 200 Ileal pouch-anal anastomosis (IPAA) surgeries per year, having performed more than 5,500 as of 2021.
- The Pouch Center's surgeons have not only completed the greatest number of pouch surgeries than any other hospital in the world, the Center also has the lowest pouch failure rate reported by any institution.
- Patients of all ages can be candidates for a pouch procedure.
- The Pouch Center sees patients from all over the world.
Several types of pouch surgeries are available to patients suffering from inflammatory bowel diseases and diseases of the colon and rectum. If you are a candidate for pouch surgery, it's important to talk with your doctor about which type of pouch surgery would be the best for your body and condition. Most patients at Cleveland Clinic receive a J-Pouch, but other pouch options are also available depending on the patient's condition and overall health.
The team also specializes in correction and management of existing pouches including: S-Pouch, K-Pouch, W-Pouch or BCIR Pouch (although not common).
In general, pouch surgery involves removal of the colon and rectum and forms a passageway with the small bowel to the anal opening. Depending on the procedure, the small bowel is folded on itself forming the shape of a "J" or "S".
About the center
Cleveland Clinic has established the world’s first and largest Pouch Center at which a variety of pouch-associated disorders, such as pouchitis (inflammation in pouch) and Crohn’s disease of the pouch, are diagnosed and successfully treated. The Center has drawn patients from all around the United States of America as well as throughout the world. The Center sees 1,000 patients annually and performs about 500 pouch endoscopies each year.
Cleveland Clinic's Digestive Disease & Surgery Institute has performed more operations for Crohn's disease as well as J-Pouch procedures than any other institution. Cleveland Clinic is recognized in the U.S. and throughout the world for its expertise and care.
Team approach
We work in collaboration with many other specialists and centers in order to provide our patients with the best outcomes. There are many key components that play into delivering quality care before, during and after surgery. Your team will tailor your plan of care to meet your individualized need and help you regain your health.
The team includes:
- Colorectal surgeons.
- Gastroenterologists.
- GI pathologists.
- GI radiologists.
- Specialists in inflammatory bowel disease.
- Nurse practitioners and physician assistants.
Nutrition support, enterostomal care (ET), pain management and physical therapy are available if needed to be incorporated into your care and recovery.
What if I need an interpreter at Cleveland Clinic?
Patients from all over the world travel to The Pouch Center for our expert care and good success. Cleveland Clinic provides interpretation services at no additional cost. Most of our interpreters have medical backgrounds and work efficiently to ensure optimal communication.
Interpreters do more than simply facilitate communications between the patient and providers and hospital staff. They help you and your family every step of the way during your medical management.
Indications for pouch surgery
When is it time to consider surgery for familial admit polyposis (FAP) or inflammatory bowel disease (IBD), specifically ulcerative colitis (UC)?
It is time to consider having pouch surgery when:
- Patients have tried every medication available to treat the disease and they have not had effective symptom resolution.
- Patients are at high risk for developing a colorectal cancer either from FAP or IBD, or they have developed dysplasia (a precancerous lesion on biopsy).
- Overall poor quality of life exists, restricting diet, sexual health, social health and trouble participating normally in work or school.
- Patients have severe ulcerative colitis, toxic megacolon and/or perforation of the colon.
How the pouch works as part of your body
How does the digestive system work following pouch surgery?
The primary job of the colon is to store stool and absorb water, while the primary job of the small intestine is to absorb nutrients, minerals and fluids. During pouch surgery, your colon and rectum are removed and a canal is formed from the end of your small bowel to your anus forming a new passageway for stool.
Nutrient and mineral absorption should not be impacted after pouch surgery (unless you have had prior small bowel resection). However, you may have issues with dehydration, if you are not diligent about keeping hydrated.
Once the pouch is formed and the stoma is closed you will likely have the urge to have a bowel movement. Most patients usually have three to nine bowel movements in a 24 hour period. Controlling and managing bowel movements will become easier as you find out what diet and foods work for you, as well as timing of when you should eat.
The stool consistency is usually semi-liquid to soft depending on diet and fluid intake. The use of antidiarrheal medications may be prescribed to help thicken the stool.
All information is provided by Cleveland Clinic Ileal Pouch Center.
Information may not be duplicated or used by other organizations or institutions without the consent or acknowledgement of Cleveland Clinic.
Contact pouchcenter@ccf.org for more information.
Types of Pouches
Commonly used names for a J-Pouch include ileal pouch and pelvic pouch. Similarly constructed ileal pouch types include the S-Pouch and K-Pouch (Kock pouch or continent ileostomy). Most patients at Cleveland Clinic receive a J-Pouch, which is the current gold standard of pouch surgical procedures.
A pouch surgery could mean a procedure involving any type of these different pouches. Your medical team will include you in a discussion about which type of pouch is best for your condition and anatomy.
Types of pouches
J-Pouch
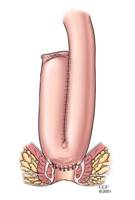
A J-Pouch (the most common type of pouch formed in pouch surgery) is constructed using two loops of the small intestine measuring approximately six inches in length. After pouch construction is complete, the pouch is capable of holding about 2/3 of a pint of fluid. Each pouch is tested using sterile saline to fill the pouch and insure the pouch is completely watertight. After testing, the pouch is placed into the pelvis where the rectum used to be and attached to the upper portion of the anal canal. This is the primary pouch procedure done within Cleveland Clinic.
All pouches need to have an annual pouchoscopy.
All pouches are susceptible to pouchitis. Pouchitis (an inflammation of the lining of the pouch) may occur after the construction of the pouch. Pouchitis (although the exact mechanism is unknown) is thought to be due to an overgrowth of bacteria in the pouch. This occurs because stool stays in contact with the ileal mucosa (lining) between bowel movements or catheterizations. Pouchitis is treated by a short course of antibiotics and usually resolves within a few days after the treatment was started. It is also advisable to assess for any other causes of pouchitis such as autoimmune, mechanical or hormonal imbalance, especially if antibiotics do not help with pouch inflammation.
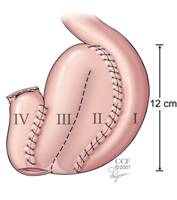
S-Pouch

An S-Pouch is constructed with three loops of the small intestine measuring about five to six inches each in length. These loops are used to construct the pouch. Each of the three loops in the small intestine is further sewn to the other forming a balloon-shaped pouch. The pouch capacity varies from 1/2 pint to just a little more than a pint when it is filled with fluid. The S-Pouch is much less commonly created during pouch surgery as most patients will undergo the creation of a J-Pouch. It is somewhat bulkier than the J-Pouch. The S-Pouch is usually avoided in individuals whose pelvis is especially narrow or small because it is slightly larger and requires a wider pelvis. The S-Pouch is attached to the top of the anal canal in the same manner as the J-Pouch.
All pouches need to have an annual pouchoscopy.
All pouches are susceptible to pouchitis. Pouchitis (an inflammation of the lining of the pouch) may occur after the construction of the pouch. Pouchitis (although the exact mechanism is unknown) is thought to be due to an overgrowth of bacteria in the pouch. This occurs because stool stays in contact with the ileal mucosa (lining) between bowel movements or catheterizations. Pouchitis is treated by a short course of antibiotics and usually resolves within a few days after the treatment was started. It is also advisable to assess for any other causes of pouchitis such as autoimmune, mechanical or hormonal imbalance, especially if antibiotics do not help with pouch inflammation.
W-Pouch
A W-Pouch is constructed using four loops of the small intestine. W-Pouches are very infrequently created and are of more historical significance. Patients with existing W-Pouches are followed and managed in the Pouch Center.
All pouches need to have an annual pouchoscopy.
All pouches are susceptible to pouchitis. Pouchitis (an inflammation of the lining of the pouch) may occur after the construction of the pouch. Pouchitis (although the exact mechanism is unknown) is thought to be due to an overgrowth of bacteria in the pouch. This occurs because stool stays in contact with the ileal mucosa (lining) between bowel movements or catheterizations. Pouchitis is treated by a short course of antibiotics and usually resolves within a few days after the treatment was started. It is also advisable to assess for any other causes of pouchitis such as autoimmune, mechanical or hormonal imbalance, especially if antibiotics do not help with pouch inflammation.
K-Pouch

The continent ileostomy is commonly known as the “K” pouch or “kock” pouch. This pouch is an option for very selected patients with ulcerative colitis when the rectum needs to be removed because of disease, if the anal sphincter muscles are weak or if previous surgery has removed the rectum and the sphincter muscles altogether. After the removal of the entire colon and rectum, the last portion of the small intestine can be used to construct an internal reservoir, which is then connected to the abdominal wall by a special ileostomy. Approximately 20 to 22 inches of the ileum is used to construct the pouch and stoma. Three loops of small bowels measuring approximately six inches each are sutured together to form the pouch. The valve or “nipple” is constructed from the six-inch segment of the ileum between the stoma and the pouch. This nipple is designed to function like a flap valve to keep feces and gas inside the pouch until it is convenient to drain the pouch. As the pouch fills with stool and gas, the pressure inside the pouch increases and a narrow opening in the center of the nipple valve closes. This prevents the escape of stool and gas until the catheter is placed into the pouch for drainage.
All pouches need to have an annual pouchoscopy.
All pouches are susceptible to pouchitis. Pouchitis (an inflammation of the lining of the pouch) may occur after the construction of the pouch. Pouchitis (although the exact mechanism is unknown) is thought to be due to an overgrowth of bacteria in the pouch. This occurs because stool stays in contact with the ileal mucosa (lining) between bowel movements or catheterizations. Pouchitis is treated by a short course of antibiotics and usually resolves within a few days after the treatment was started. It is also advisable to assess for any other causes of pouchitis such as autoimmune, mechanical or hormonal imbalance, especially if antibiotics do not help with pouch inflammation.
Patient FAQ’s
What will my diet be like with a K-Pouch?
Similar to other pouches, you will want to monitor the intake of carbohydrates and fiber. It is important to figure out the threshold that regulates your bowel frequency at an ideal level.
Every patient is different in tolerating certain kinds of food. Keep a food journal and modify one thing at a time in your diet. Keep track of the food and your subsequent bowel frequency after consumption. This is a good way to tell what foods you can tolerate and what foods you cannot. The food journal also helps to regulate postprandial abdominal bloating and/or pain.
How do I use the restroom with a K-Pouch?
The K-Pouch needs to be emptied using a catheter. The right size and caliber of catheter needs to be optimized for every individual patient. It will be helpful to carry with you a kit that contains lubricant for the catheter and some clean bandages to cover the stoma of the K-Pouch. Stoma nurses will guide you more in this regard. It will be advisable to have multiple replicas of kits, so you will have a backup if needed. You should avoid using any alternative other than the catheter, such as plastic straw or hard tube. This practice will prevent any trauma or harm to the pouch.
What will be the major limitations I will need to overcome with a K-Pouch?
Avoid intubation trauma and be patient while emptying the pouch. Avoid gaining excessive weight, mainly on the belly to protect the nipple valve of the pouch.
BCIR (Barnett Continent Intestinal Reservoir)
A BCIR is a surgical pouch infrequently created after surgical treatment for IBD or colorectal cancer. Although this type of pouch procedure is not offered at Cleveland Clinic, revision surgery is sometimes offered to patients with an existing BCIR.
All pouches need to have an annual pouchoscopy.
All pouches are susceptible to pouchitis. Pouchitis (an inflammation of the lining of the pouch) may occur after the construction of the pouch. Pouchitis (although the exact mechanism is unknown) is thought to be due to an overgrowth of bacteria in the pouch. This occurs because stool stays in contact with the ileal mucosa (lining) between bowel movements or catheterizations. Pouchitis is treated by a short course of antibiotics and usually resolves within a few days after the treatment was started. It is also advisable to assess for any other causes of pouchitis such as autoimmune, mechanical or hormonal imbalance, especially if antibiotics do not help with pouch inflammation.
All information is provided by Cleveland Clinic Ileal Pouch Center.
Information may not be duplicated or used by other organizations or institutions without the consent or acknowledgment of Cleveland Clinic.
Contact pouchcenter@ccf.org for more information.
Our Doctors
Looking for a gastroenterologist?
Find A ProviderPatient Referrals
Referring physician hotline: 855.REFER.123 or 855.733.3712
Cleveland Clinic’s Referring Physician Center has established a hotline, available from 7 a.m. to 7 p.m. EST, every day, for referring physicians and their office staff to streamline access to our array of medical services. Our goal is to make it as easy as possible for you and your patients when you entrust us with their care.
Contact the Referring Physician Hotline to obtain information on our clinical specialists and services; schedule and confirm patient appointments; receive assistance in the resolution of any service-related issues; and connect with Cleveland Clinic specialists.
When contacting us to schedule your patients, please have the following information readily available:
- Patient demographic information.
- Reason for visit.
- Any special needs that will require facilitation once the patient arrives.
- Patient insurance information, if available.
We will work with your patient to complete the registration process and to schedule an appointment at the patient's convenience. You will be notified once the appointment is scheduled.
The Referring Physician Hotline can be reached from 7 a.m. to 7 p.m. EST, every day, by calling 855.REFER.123 (855.733.3712).
All information is provided by Cleveland Clinic Ileal Pouch Center.
Information may not be duplicated or used by other organizations or institutions without the consent or acknowledgement of Cleveland Clinic.
Contact pouchcenter@ccf.org for more information.
Contact Us
Cleveland Clinic Ileal Pouch Center
A Building (Crile Building) 31
9500 Euclid Avenue
Cleveland, OH 44195
Appointments
To schedule an appointment in our Digestive Disease & Surgery Institute please call 216.444.7000 (or toll-free 1.800.223.2273, ext. 47000)
Ask a question
If you are experiencing a medical emergency, please call 9-1-1 or go to the nearest emergency room. Also we cannot provide a specific medical opinion or answer without a clinical consultation. If you would like to speak with a Cleveland Clinic Representative, please call 800.223.2273
All information is provided by Cleveland Clinic Ileal Pouch Center.
Information may not be duplicated or used by other organizations or institutions without the consent or acknowledgement of Cleveland Clinic.
Contact pouchcenter@ccf.org for more information.
Resources
J-Pouch Treatment Guide
This guide aids patients in understanding how a J-Pouch is created, addresses who may be a candidate for a J-Pouch, and identifies the benefits of the procedure.
- Call 216.444.7000 to schedule an appointment.
- Download the guide.
Download information pamphlets
WOC nursing
The Wound, Ostomy and Continence (WOC) nursing department helps patients with pouch surgery learn to take care of themselves until they feel comfortable.
Learning to live and adjust to life after having a pouch surgery can be difficult at first. Some people may adjust faster than others, while some may experience complications. It's about finding out what works best for you.
Cleveland Clinic has prepared many helpful resources for patients in all different stages of pouch surgery. There are also many other online resources available to the pouch community, however none of these resources are as valuable as discussing your concerns or questions with your physician.
Online resources
The Crohn's and Colitis Foundation of America (CCFA) is a non-profit, volunteer-driven organization dedicated to finding the cures for Crohn's Disease and ulcerative colitis.
- Visit CCFA's website (link will open in a new tab/window).
The mission of Girls With Guts is to empower girls and women with Inflammatory Bowel Disease (Crohn’s Disease & ulcerative colitis) and ostomies to share their stories of confidence and to promote self-esteem.
- Visit Girls with Guts website (link will open in a new tab/window).
Cleveland Clinic Dehydration Clinic
If you are experiencing symptoms of dehydration before 2 p.m. please contact an endoscopy nurse within our Digestive Disease & Surgery Institute. If you are in stable condition, one of our staff members may recommend that you come in to get intravenous fluids and electrolytes, usually in the form of an IV.
What are signs and symptoms of dehydration?
- A dry mouth or lips.
- Thirsty feeling.
- Tiredness.
- Confusion.
- Light headedness or dizziness.
- Sunken eyes.
- Reduced tears.
- Muscle cramps.
- Decreased frequency and/or quantity of urination with dark colored urine.
What should I do if I am dehydrated?
Contact our Dehydration Clinic if you are local. If not, please call your primary care provider or approach the ER immediately. Mild dehydration can be treated at home by drinking lots of fluids such as Pedialyte, Pediasure or Gatorade. Mild dehydration can progress to moderate to severe dehydration if not addressed earlier. It is very important to assess and treat the cause of dehydration, so seek consultation with your gastroenterologist.
Can I prevent dehydration?
Yes! It can be prevented by drinking plenty of fluids. It is essential to get electrolytes.
