An arrhythmia is a heart rhythm that isn’t normal. Your heart may be beating too fast or too slow, or just not beating in a regular pattern. Arrhythmias range from harmless to serious, with symptoms and without. There are many options to treat arrhythmias, but some don’t need them. The prognosis varies greatly depending on the type.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
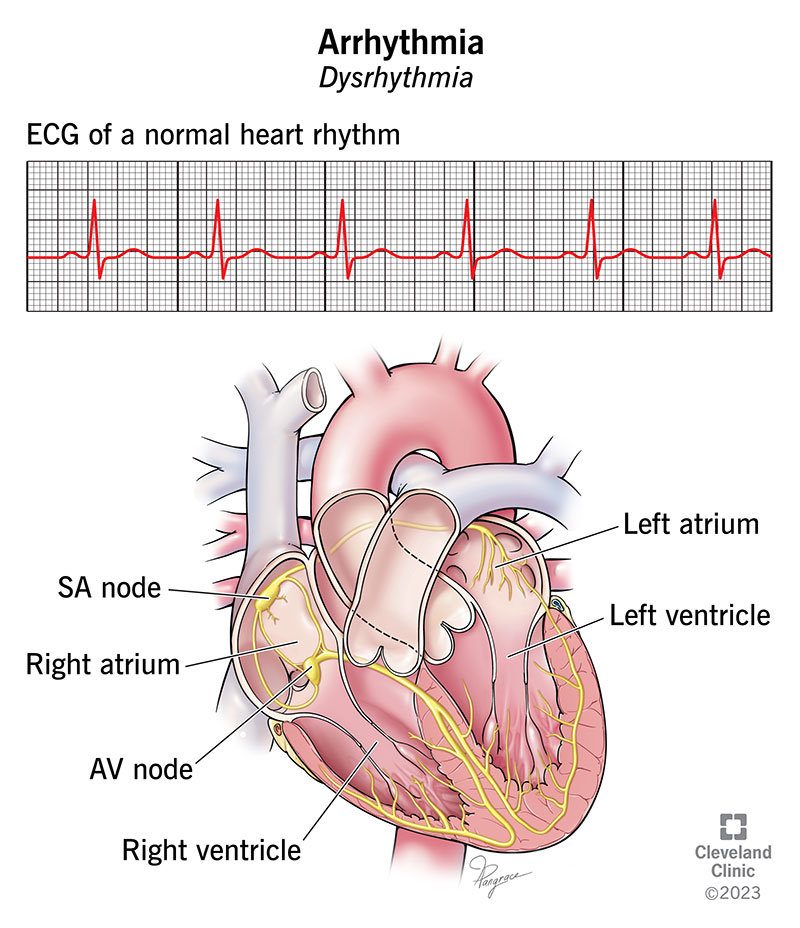
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/16749-arrhythmia-illustration)
An arrhythmia is a problem with your heart’s rhythm. It happens when electric signals that tell your heart to beat don’t work the way they should. As a result, your heart may beat too fast, too slow or just irregularly. You may feel like your heart is racing, fluttering, pounding, skipping beats or adding extra beats.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Normally, your heart beats in a steady, organized rhythm. Issues with various parts of your heart or abnormal blood flow to your heart can affect your heart’s normal rhythm. Having a normal heart rhythm matters because your heart supplies your whole body with nutrients and oxygen through the blood it pumps. Having an abnormal rhythm may hinder this.
Up to 5 out of 100 people may have arrhythmias. Some don’t have symptoms, which makes it difficult to know how many people actually have this condition. In the U.S., atrial fibrillation is the most common type of cardiac arrhythmia.
Some types of arrhythmias are harmless and don’t require treatment. Other types can put you at risk for cardiac arrest. Many are in between these two extremes. Most arrhythmias in children are self-limited, but some may need additional treatment or close follow-up. A healthcare provider can tell you which type of arrhythmia you have and what kind of treatment you need, if any.
Healthcare providers describe arrhythmias by where in your heart they start. These types include:
Advertisement
A cardiac arrhythmia may not cause any symptoms. In rare cases, the first symptom may be a seizure or sudden cardiac death.
Heart arrhythmia symptoms may include:
Most arrhythmias happen because of an issue with your heart’s arteries, valves or muscles. Causes of arrhythmia in adults and children include:
Adults and children can have cardiac arrhythmias. Risk factors include:
Here are some ways to lower your risk of arrhythmia:
Without treatment, heart arrhythmias can lead to complications, like:
A healthcare provider can find an irregular heartbeat by taking your pulse and listening to your heart. After reviewing your symptoms and performing a physical exam, they may order diagnostic tests to help confirm that you have an arrhythmia. This can also help find the cause.
You may also see an electrophysiologist. This is a heart expert who has extra training in diagnosing and treating heart rhythm disorders.
Some tests that can check for an irregular heart rhythm and related diseases include:
Advertisement
Heart arrhythmia treatment depends on the type and severity of your heart rhythm. In some cases, you don’t need any treatment. Options include:
Many medications can treat heart arrhythmias. Because everyone is different, you may have to try several medications and doses to find the one that works best for you. Medicines include:
Simple changes to the way you live can help with arrhythmias. These changes may include:
In addition to medicine, some people need procedures to treat abnormal heart rhythms. Your healthcare provider will determine the best treatment for you and discuss the benefits and risks of these with you.
Advertisement
Procedures include:
A cardiologist may insert certain devices during a procedure in the electrophysiology lab. Devices to treat a heart arrhythmia include:
If you have an arrhythmia, you may need heart surgery for any of these reasons:
Advertisement
Depending on the procedure or surgery, recovery afterward can take weeks or months. If you have a procedure like catheter ablation or pulmonary vein isolation, you may still have arrhythmias for several weeks while you’re healing. Your provider can tell you what to expect.
Your provider will tell you how often you should visit. Call them in between visits if your symptoms become more frequent or severe.
You’ll need to visit your provider for regular follow-up visits to:
Get immediate medical care if you have:
Questions to ask your provider may include:
Depending on the type of cardiac arrhythmia you have, you may have mild or severe symptoms or none at all. You may not need treatment, but some people need medicine or a procedure. With heart arrhythmia treatment, many people can live full lives. Some people with more serious arrhythmias may have a cardiac arrest and may or may not survive.
Harmless arrhythmias go away and come back in response to what triggers them. But people with other types of arrhythmias — especially those that put you at risk for cardiac arrest — need treatment for the rest of their lives.
Most types of irregular heartbeat in children are harmless. And most go away with treatment of the underlying cause, like a fever or infection. But some types can be serious.
If you or your child experiences arrhythmia symptoms, a Valsalva maneuver may help. You can do this by:
Boring is good when it comes to your heart rhythm. But an arrhythmia, or abnormal heart rhythm, can be unsettling. It’s important to see a healthcare provider if you have symptoms like shortness of breath or heart palpitations. They’ll help find the best treatment option for you. It may also be a good idea to tell family and friends what your symptoms look like and when to call for emergency help.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When your heart rhythm is out of sync, the experts at Cleveland Clinic can find out why. We offer personalized care for all types of arrhythmias.
