Depression is a common mental health condition that affects how you feel, think and function each day. It can cause ongoing sadness, low energy and loss of interest in things you once enjoyed. With the right treatment, including therapy or medication, many people start to feel better.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Depression is a common and serious mood disorder that causes ongoing sadness and a loss of interest in things you once enjoyed. It can affect how you eat, sleep and think.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
It’s normal to feel sad or have a low mood after difficult life events, like losing a job or a breakup. But depression is different. It lasts most of the day, nearly every day, for at least two weeks. It affects how you function. And it can lead to serious complications, like suicidal thoughts and behavior.
About 3 in 10 adults receive this diagnosis at some point in their lives. But the true number may be higher. Many people don’t seek medical help for their symptoms and may not get diagnosed.
Depression is treatable with therapy, medication or both. A mental health provider can help you feel better.
According to the DSM-5, the main types are:
Advertisement
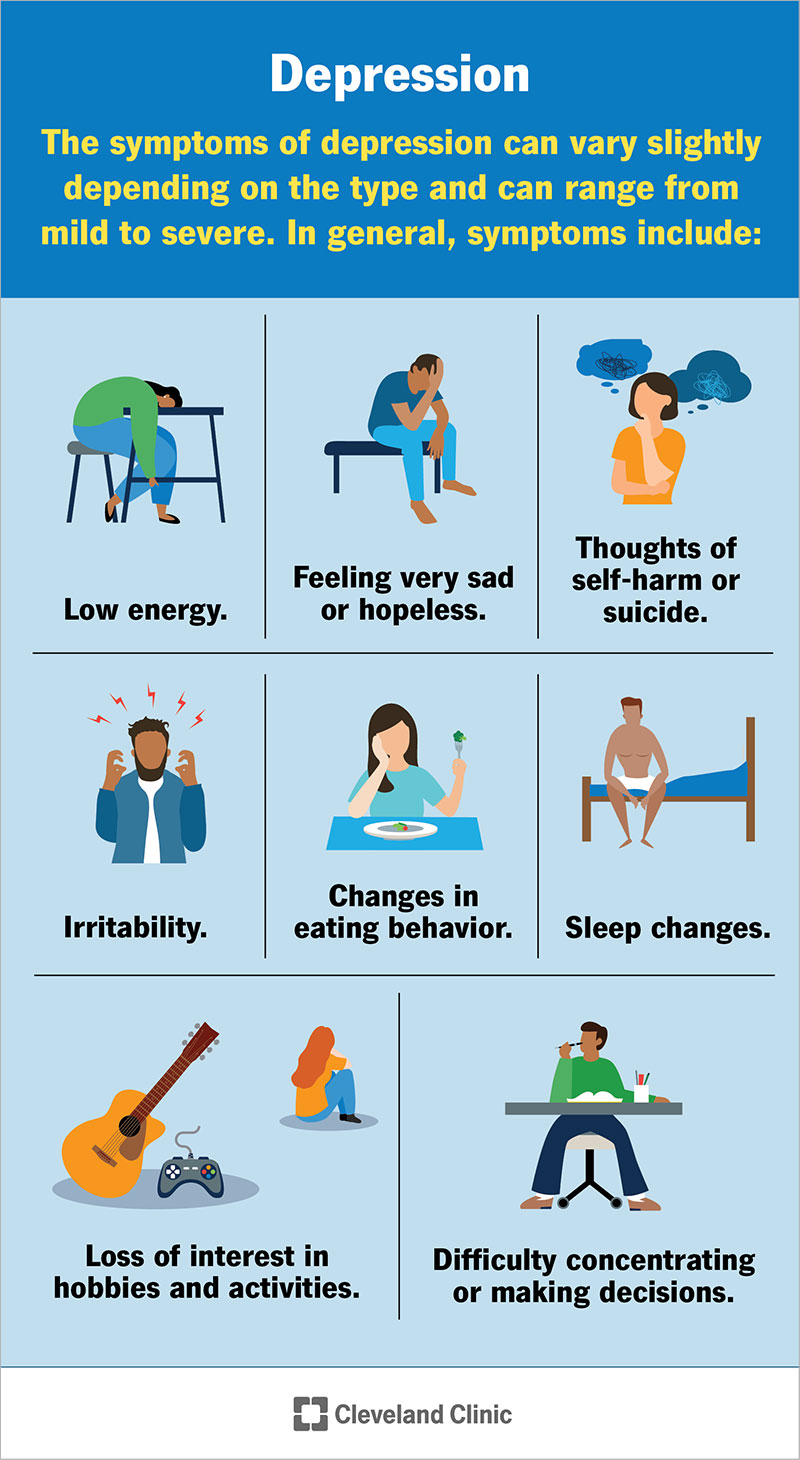
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/9290-depression)
Depression may affect how you feel, think and function day to day. Common symptoms include:
These symptoms can start slowly. Sometimes, a loved one may see changes in your mood or behavior before you do. If you notice these signs in yourself or someone you care about, check in and consider getting support.
Each case of depression is slightly different. But many people describe feeling a constant weight that doesn’t lift. Sadness or hopelessness may color most of your thoughts. Sometimes, it doesn’t feel like sadness at all. It might feel like numbness or a lack of emotion. You may also feel more easily frustrated than usual.
Things you once enjoyed may no longer feel interesting or worth the effort. You might stop doing hobbies and pull away from friends. Even small tasks, like getting dressed or starting your day, can feel exhausting and take much more energy than before.
Over time, your thoughts may become more negative. You might feel guilty, worthless or blame yourself for things that aren’t your fault. You may also have thoughts about death or not wanting to wake up. This is a major sign that you need medical help.
It’s important to remember that this is a treatable mental health condition and help is available.
Depression doesn’t have a single cause. It usually develops from a mix of factors, like:
You can’t always prevent depression. But you can try to reduce your risk by keeping a regular sleep routine and managing stress in healthy ways. Self-care activities, like exercise, meditation or yoga, can help, too.
Having certain risk factors can make it more likely that you may develop depression. For example, the following conditions are associated with higher rates of depression:
Advertisement
Depression can affect many areas of your life and health over time. Possible complications include:
If you or a loved one is thinking about suicide, dial 988 on your phone to reach the Suicide and Crisis Lifeline (U.S.). Someone is available to help you 24/7.
A healthcare provider will diagnose depression by going over your symptoms and medical history. Providers look for at least two weeks of low mood and/or loss of interest, along with other symptoms that affect your daily life.
Your provider will also rule out other possible causes, like medical conditions, medications or substance use. They may ask about your sleep, appetite, energy and stress.
There isn’t a lab test or scan that can diagnose depression. Instead, your provider may use questionnaires and basic medical tests to better understand your symptoms. These help guide diagnosis and treatment, but they don’t diagnose depression on their own.
Advertisement
Common tools include:
They’ll compare these results to the diagnostic criteria in the DSM-5. This is a professional reference book on mental health conditions.
Healthcare providers don’t describe depression in stages. Instead, your provider may describe it based on severity, such as mild, moderate or severe. They may also refer to it as a first episode, recurring or long-term (persistent).
Treatment for depression usually involves talk therapy, medication or a combination of both. Other options may help. Your provider will help you choose the best approach.
Talk therapy (psychotherapy) involves talking with a mental health professional. They can help you understand your thoughts, feelings and behaviors. You learn ways to cope. Different types of therapy that may help depression include:
Advertisement
Antidepressants may help with symptoms. These medications affect brain chemicals that regulate your mood.
Common types include:
Your provider will help choose the right medication based on your symptoms and health history.
In some cases, additional treatments may help, like:
With proper diagnosis and treatment, most people with depression live healthy, fulfilling lives. Depression can return after you get treatment, though. It’s important to seek medical help as soon as symptoms begin again.
Without treatment, depression can:
It’s important to remember that support is available, no matter where you are or what you’re going through.
How long depression lasts can vary. It often depends on factors like how severe your symptoms are, the support you have and the type of treatment you receive. There isn’t a set timeline for everyone.
Symptoms may last for weeks, months or longer. Even with treatment, they may not go away right away. You may also notice some lingering symptoms as you start to feel better.
Depression may feel heavy in a way that’s hard to put into words. It can quietly change how you move through your day, how you connect with others and how you see yourself.
If any of the symptoms sound familiar, get help. These feelings aren’t something you just have to push through on your own. Support — whether that’s talking with a provider, starting therapy or exploring other treatment options — can help lighten that weight over time.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Depression can hamper every aspect of your life. Cleveland Clinic experts are here to help manage your mental health so you can do the things you want.
