Hypomania causes high energy, mood changes, impulsive behavior and little need for sleep. It’s less intense than mania, but still noticeable to others. It’s often part of bipolar disorder, but it can also happen with other conditions. You can manage it with medication, therapy and self-care.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
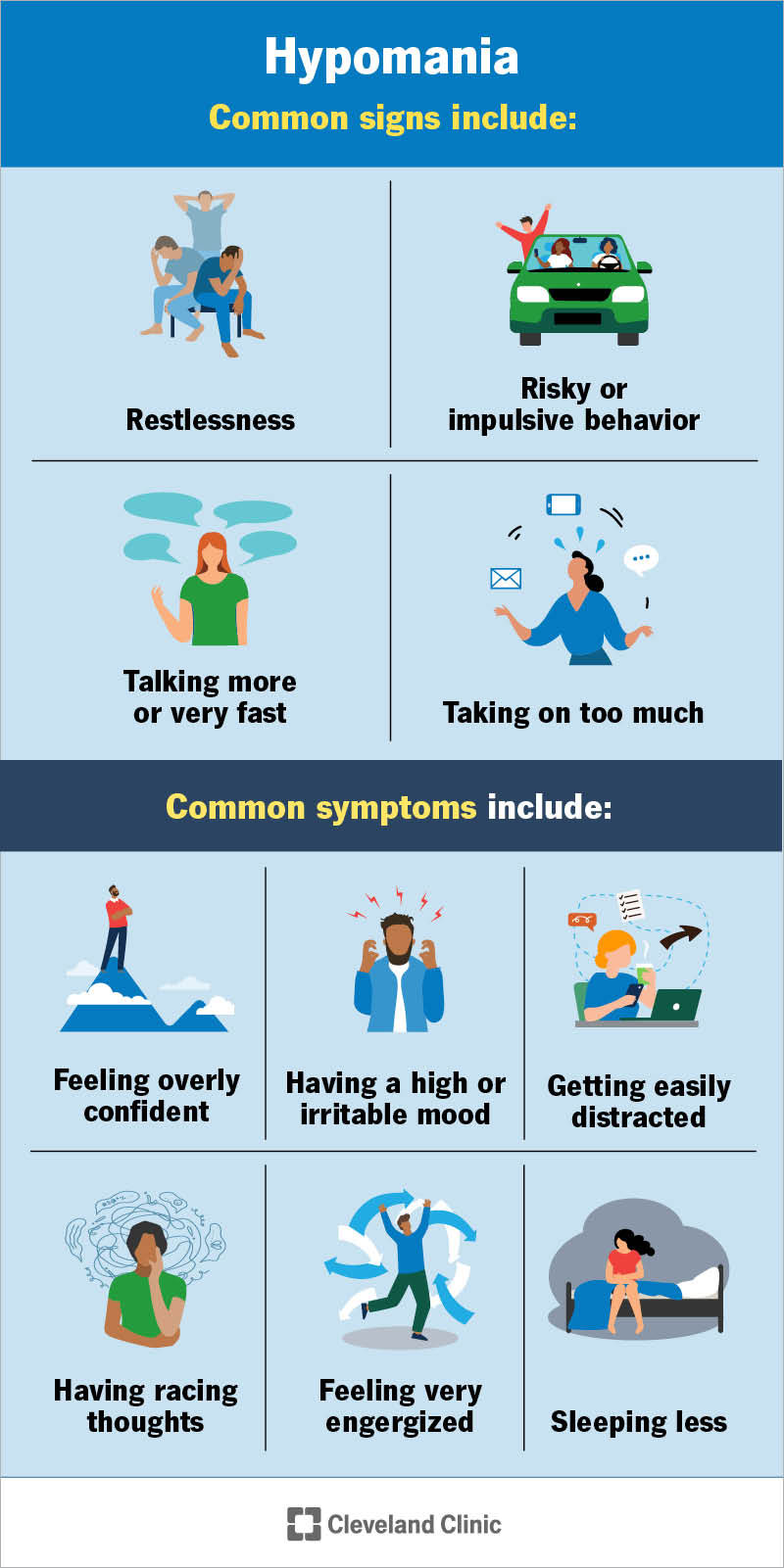
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/hypomania)
Hypomania happens when your mood, energy and activity level become higher than usual. It’s shorter and less severe than mania (manic episodes).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
You may need little sleep, talk more or feel like you can take on many tasks at once. You may also feel unusually confident or even invincible. These changes are different from your normal self and noticeable to others. Hypomania usually doesn’t cause major problems in your daily life and doesn’t typically require hospital care.
Hypomania is a symptom of bipolar disorder, but it can also appear in other conditions. A healthcare provider can help you understand the cause and find the right treatment.
A hypomanic episode is the active period when your mood, behavior and energy level are much higher than usual. Symptoms last most of the day, almost every day, for at least four days in a row.
Even though the symptoms are less severe and may not disrupt your daily life as much as mania, they may still put you at risk of harm.
Hypomania can build slowly, so you may not notice the changes at first. Loved ones often see the shift before you do. Common signs include:
Advertisement
The experience of hypomania can vary from person to person. Common symptoms include:
After a hypomanic episode, you may feel:
Researchers don’t fully understand the exact cause of hypomania. They believe it develops from a mix of genetic factors, brain chemistry and life experiences. These can affect how your brain regulates mood, energy and judgment.
You may have a higher chance of having hypomania if you live with a mental health disorder (like bipolar II disorder or cyclothymia) or have relatives with bipolar disorder. You may also have a higher risk if you have a brain injury, brain tumor or stroke.
Certain things may increase the chance of a hypomanic episode. These triggers can vary from person to person. Some common triggers include:
A healthcare provider can help you identify what may be triggering symptoms.
Your healthcare provider will start by asking about your medical history and your biological family’s health background. They’ll also review all the medicines, supplements and herbal products you use. They may order blood tests, urine tests or imaging studies to rule out other medical issues that can look like hypomania.
If they don’t see a physical cause, your provider may connect you with a mental health provider to make a diagnosis.
A mental health provider uses the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to decide if your symptoms meet the definition of hypomania.
Advertisement
To diagnose this symptom and its cause, your provider looks for:
Your provider may also look at how your symptoms responded to past treatments. They’ll use all of this information to make the most accurate diagnosis.
Treatment is personalized for hypomania. Your provider might recommend medications, therapy, self-care or a combination of these to manage symptoms.
Advertisement
Your provider might offer different medications to manage hypomania. These may include:
Talk with your provider about possible side effects before starting any medication. They’ll explain what to watch for and help you choose what’s safest for you. Some medicines may be unsafe if you’re pregnant or planning to become pregnant.
Your provider may suggest talk therapy to help you understand why this symptom happens and to build skills that make it easier to manage. Different kinds of therapy may be helpful:
Your provider may encourage you to focus on self-care to help keep your mood as steady as possible. You may find these steps helpful:
Advertisement
An episode lasts at least four days. It can continue for several weeks or longer. The length depends on the underlying cause. Treatment may reduce the length.
You should call your provider if symptoms:
Getting help early may keep it from turning into a more serious manic episode or leading to harmful consequences.
Contact your provider right away if you have suicidal thoughts. You can always reach out to the Suicide and Crisis Lifeline at 988 (U.S., call or text). Someone is available 24/7.
Hypomania can be tricky. It might feel like you’re finally catching up — more energy, more ideas, less sleep. But what feels productive or exciting at first might quietly shift into something harder to manage, especially if it leads to risky decisions or burnout.
It helps to remember that hypomania is a symptom, not a personal flaw. Recognizing early signs gives you a chance to slow things down and protect your health. That might mean adjusting your routine, checking in with a provider or asking someone close to help you keep an eye on your behavior.
With the right support and strategies, it’s possible to manage hypomania and its underlying cause so you can maintain balance. Keep paying attention to what your body and mind are telling you — and reach out when something feels off.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Your mental well-being is just as important as your physical well-being. Cleveland Clinic’s mental health experts can help you live life to the fullest.
