Alpha-1 antitrypsin deficiency is a genetic condition that can cause lung and liver damage. It happens when a gene change causes low levels of AAT, a protein that protects your lungs. Common symptoms include chronic cough, shortness of breath and wheezing. Not smoking is the best way to reduce your risk of serious complications.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
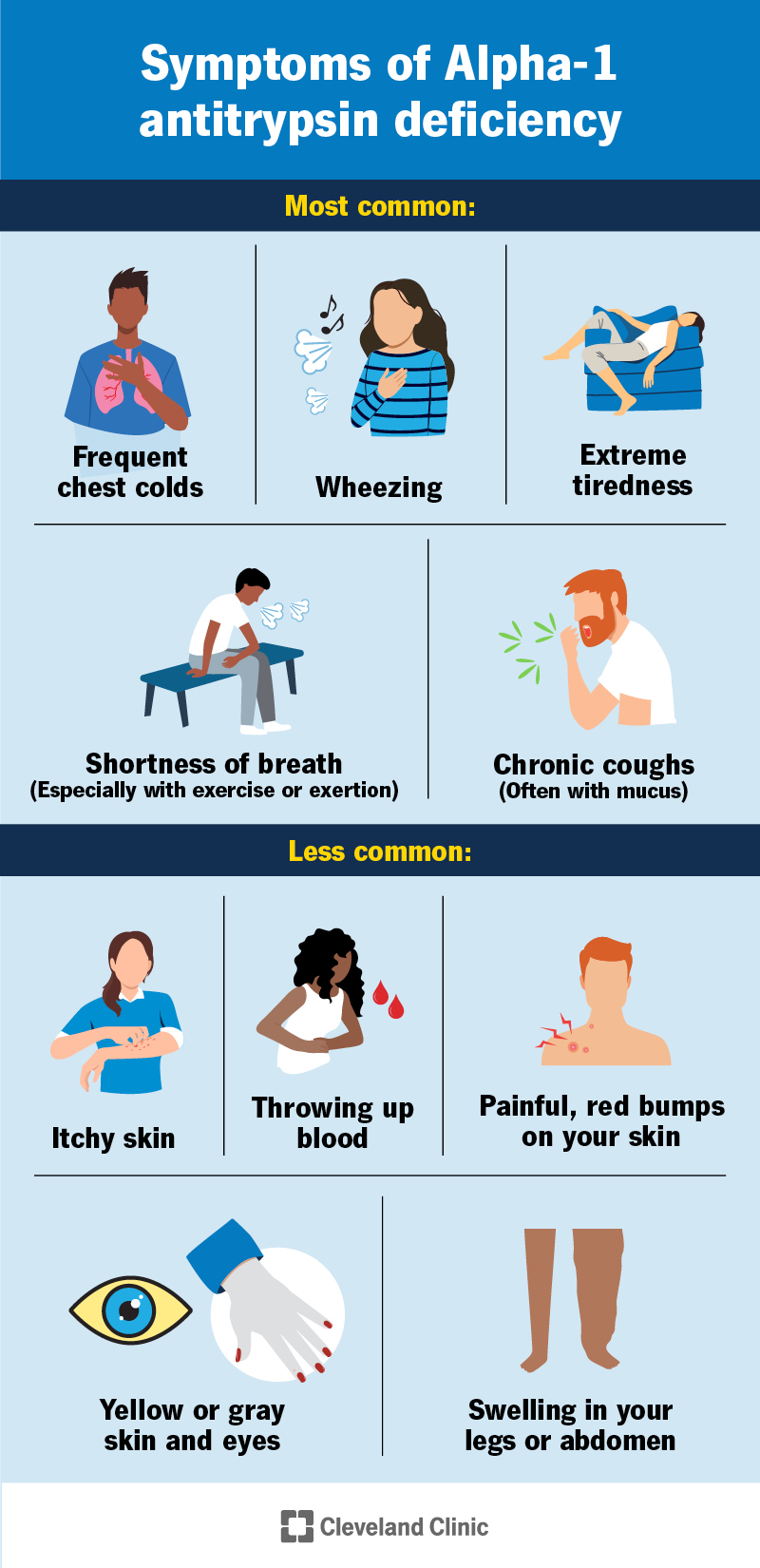
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/alpha-1-antitrypsin-deficiency)
Alpha-1 antitrypsin deficiency (or just “Alpha-1”) is a genetic disorder that increases your risk of developing lung disease and liver damage. It happens when a gene change causes low levels of alpha-1 antitrypsin (AAT), a protein that protects your lungs from damage. It can also cause a buildup of AAT in your liver.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
If you have Alpha-1, you’re at increased risk for:
Some of these conditions can be life-threatening. Alpha-1 is sometimes called “genetic COPD” (chronic obstructive pulmonary disease) or “genetic emphysema.”
The most common symptoms of Alpha-1 affect your lungs, including:
Lung symptoms usually start between the ages of 30 and 50, but can also start later.
Some people with Alpha-1 develop liver disease, either as infants or in adulthood. Symptoms could include:
Rarely, the first symptom of Alpha-1 is painful, red bumps on your skin.
A gene change you’re born with causes Alpha-1. Changes in the SERPINA1 gene affect how your body makes Alpha-1 antitrypsin (AAT) proteins. Some changes cause AAT to form incorrectly, some tell your body to make less AAT and some tell your body not to make any at all.
Advertisement
AAT forms in your liver and moves through your bloodstream to your lungs. It’s the “off switch” for an enzyme called neutrophil elastase. Neutrophil elastase is important for fighting infections in your lungs. After elastase has had time to do its job, AAT shuts it off. This prevents elastase from accidentally damaging healthy tissues in your lungs.
Improperly formed AAT can’t move out of your liver. It builds up there and can cause scarring. It’s also not able to move to your bloodstream and your lungs to do its job.
If you have low levels of AAT or AAT that can’t get out of your liver, you won’t have enough in your lungs to stop elastase. Elastase will start breaking down the protein elastin in your lungs. Elastin gives strength to the small air sacs of your lungs (alveoli). It allows them to stretch and contract, like a rubber band. Without it, your alveoli lose their shape and become floppy (emphysema). This makes it so you can’t breathe or get oxygen properly.
Alpha-1 antitrypsin deficiency is most common in people of European ancestry. People who have two malfunctioning copies of the SERPINA1 gene are at high risk for lung disease. Smoking increases this risk.
You can also have symptoms if you have one abnormal copy of the gene and one normal copy. If you have one abnormal copy of the gene, you’re at an increased risk of lung damage, especially if you smoke or breathe in harmful substances. One in 25 people of European descent has at least one abnormal copy of the gene for Alpha-1.
Alpha-1 is an inherited condition. That means that you can pass the gene changes that cause it to your biological children. This is true if one or both copies of your SERPINA1 genes have changes.
Complications of Alpha-1 include:
Healthcare providers diagnose Alpha-1 with blood tests. Because it shares symptoms with other illnesses, sometimes it can take a long time to diagnose. Your provider might test you for it if you have liver symptoms or if you have COPD.
Your provider might do tests or procedures to measure AAT levels, determine how well your lungs or liver are working, and identify damage to your lungs or liver. Tests could include:
If you have Alpha-1, your provider may also recommend testing for hepatitis C.
Depending on how Alpha-1 affects you, treatment options may include:
Advertisement
Early diagnosis is important. Talk to your provider about testing if you have:
Advertisement
If you’ve been diagnosed with Alpha-1, see your provider if you:
Some people with Alpha-1 never have symptoms or related organ damage, especially if they never smoke. Others can have life-threatening complications. Your provider can tell you what to expect in your specific situation. Working with your provider can help you manage any conditions you have to stay as healthy as possible.
The life expectancy of someone with Alpha-1 varies widely from person to person. It may not affect how long you live. But some people have life-threatening complications. Your prognosis will depend on:
Because you’re born with the gene changes that cause it, you can’t prevent Alpha-1. But not everyone with Alpha-1 goes on to have lung and liver conditions. There are several things you can do to reduce your risk of organ damage. These include:
Advertisement
If you have Alpha-1 or are a carrier and want to have children, you may want to speak with a genetic counselor. They can help you understand the risk of passing genetic changes to your child.
Some people with Alpha-1 antitrypsin deficiency (Alpha-1) have few or no symptoms, while others have life-threatening complications. Having honest conversations with your healthcare provider can help you understand what to expect in your specific case. Together, you can make a plan to improve your symptoms, reduce your risk of complications and have the best quality of life.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When you need care for your child’s vision, it’s important to find someone you trust. Cleveland Clinic Children's experts focus on your child's needs.
