Eye herpes is a condition that can happen with very common, highly contagious viruses. Those viruses cause cold sores around your mouth, and chickenpox/shingles elsewhere on your body. These viruses aren’t curable, but treatment can limit their effects, prevent permanent vision loss and avoid future flare-ups.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
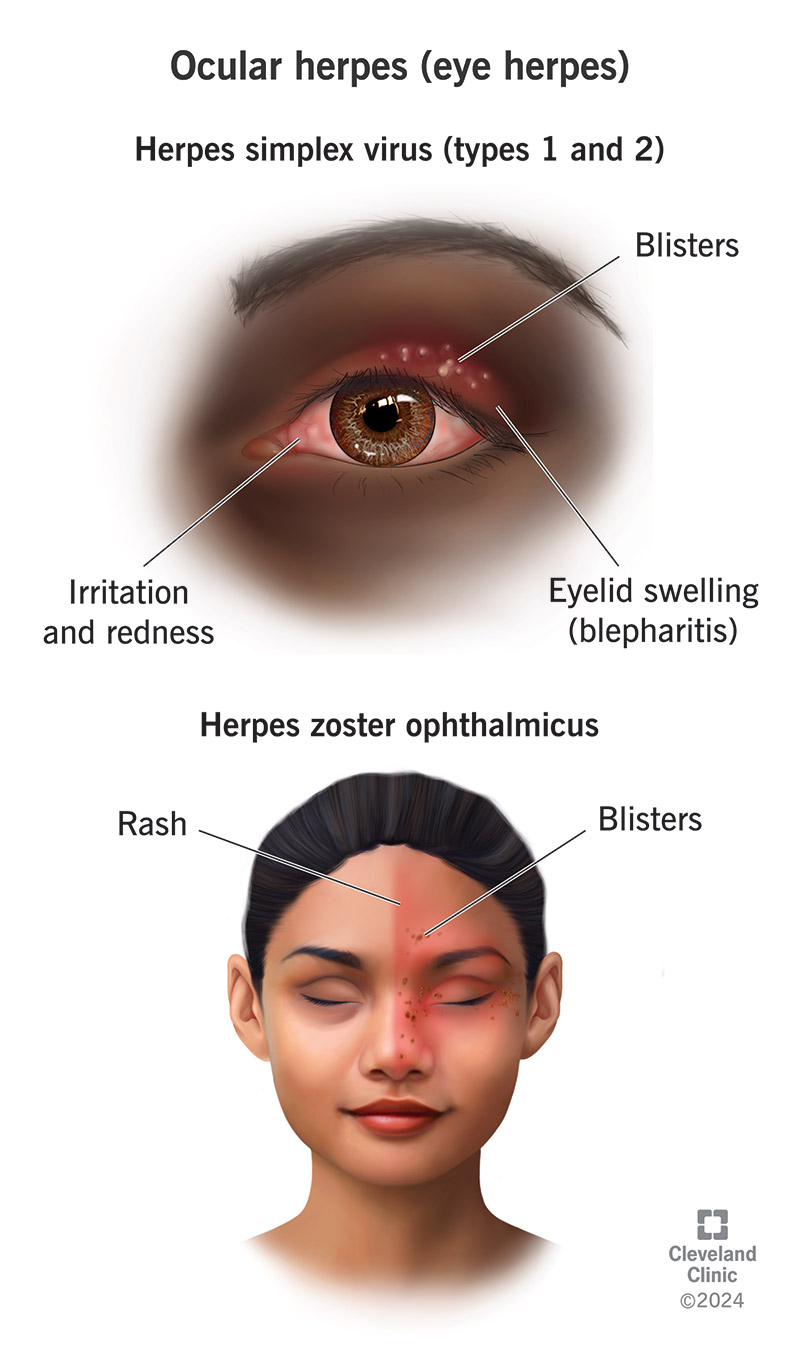
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/ocular-herpes)
Ocular herpes is when herpes viruses affect your eyes. It’s a serious and often severe condition that can cause blindness, so it needs quick diagnosis and treatment. It’s sometimes known as “herpetic eye disease” or, informally, “eye herpes.”
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
There are two main viruses that cause this condition:
About 500,000 people in the U.S. have HSV-related eye herpes, with about 58,000 cases diagnosed per year. It can affect people of any age. Because HSV is very common, many more people are at risk. Research indicates that among people in the U.S. ages 15 to 49, around 50% have HSV-1 (either active or inactive), and about 12% have HSV-2.
Varicella zoster virus affects about 1 in 1,000 people in the U.S. each year, and that number climbs to around 1 in 100 people older than 60. Experts estimate that between 8% and 20% of these cases cause eye-related symptoms and issues. Cases in children are rare.
The symptoms of eye herpes can vary slightly depending on which virus causes it, and most are symptoms that can happen with several other conditions. Some symptoms affect the eye itself, while others affect the surrounding parts of your face, too. It usually affects one eye at a time but can sometimes affect both simultaneously.
Advertisement
Typical symptoms of HSV-related herpes include:
More severe symptoms can include:
Varicella zoster can cause many eye symptoms. But it also commonly causes skin symptoms around your eye, particularly on your forehead. The virus mainly attacks your nervous system, and the trigeminal nerve branches in your forehead are a common place for those symptoms to appear.
Eye symptoms can include:
Skin symptoms usually affect one side of your face and may include:
People with varicella zoster-related eye herpes usually have general symptoms like nerve pain, fatigue or malaise (a general “unwell” feeling) before any visible eye or skin symptoms appear.
Eye herpes can happen with two strains of herpes simplex (types 1 and 2) or the varicella zoster virus. These viruses are highly contagious, meaning it’s very easy for you to catch them from other people. But there are a few important differences in how that can happen with herpes viruses and the varicella zoster virus.
It’s easy for oral herpes to spread to your eyes from your hands (for example, you touch an open sore on your lip and then touch your eye). It can cause eye herpes when it first infects you (primary infection). But it’s more common for it to affect your eyes (either traveling through your nerves or spreading via your hands) when the virus reactivates.
HSV-1 spreads easily between people through infected saliva and other bodily fluids. That can happen directly through person-to-person contact like kissing. It can also happen indirectly through shared objects like eating and drinking utensils, hygiene items, makeup and others).
Advertisement
Oral herpes commonly causes sores or blisters (sometimes called “cold sores” or “fever blisters”) on your lips or around your mouth. But the initial infection can sometimes look like an upper respiratory illness or another viral condition like mononucleosis (especially in adults).
After your immune system reacts to HSV-1, the virus can go dormant and hide in your nervous system. It can then reactivate and cause a symptomatic infection (and potentially eye herpes) later.
HSV-2 is mainly a sexually transmitted infection (STI). But in uncommon cases, HSV-2 can spread through bodily fluids to your face or eyes (either via your hands or directly). This can cause ocular herpes in babies and young children.
It's also possible to pass HSV-2 to your baby during pregnancy or childbirth. Experts call this “vertical transmission.” It’s one of the main ways that newborns can contract (catch) HSV-2 and later develop eye herpes. Research shows vertical transmission happens in about 1 in every 3,200 births each year.
Varicella zoster causes chickenpox in children and adults. Once you have chickenpox, the varicella zoster virus goes dormant and hides in your nervous system (just like HSV does). It can then reactivate at some point later in your life — sometimes years or even decades later — and cause shingles. Shingles can spread through your nervous system and reach your eyes through nerves that pass close by.
Advertisement
While the varicella zoster virus causes both chickenpox and shingles, it’s only shingles that can cause eye herpes. It’s rare for chickenpox to affect your eyes, and experts don’t classify it as eye herpes when it does. Eye herpes also isn’t contagious like shingles on your skin.
Yes, you can have eye herpes more than once. Several potential risk factors may contribute to flare-ups. They include:
The most serious complication of eye herpes is vision loss or blindness. Both types of HSV and varicella zoster can damage structures throughout your eyes. Most of the time they affect the cornea, but they can also affect the uvea and the retina. Recurrences (when the virus reactivates) can cause scarring, which leads to permanent vision loss. That’s why eye herpes is a condition that needs quick diagnosis and treatment.
Your eye care specialist will look at the skin on your eyelid and around your eye, taking note of any blisters, color changes, etc. They’ll also ask questions about your medical history and recent events that could be relevant to your infection.
Advertisement
If a healthcare provider hasn’t previously diagnosed you with a herpes simplex or varicella zoster infection, there are several ways to test for these viruses. Those range from simple swabs of your eye surface to blood tests (either for current infection or antibodies from a past infection).
An eye care specialist can also use other methods, including an eye exam, to determine the exact eye structures affected and how to treat the infection. One part of a standard eye exam, the slit lamp exam, lets your eye care specialist see inside your eye. That can help them determine the best way to treat this condition. You may also need to see a primary care provider (PCP) or another clinician for a physical exam and treatment of HSV or shingles-related effects outside your eyes.
Because so many different tests and methods can help in diagnosing and treating eye herpes, your eye care specialist is the best source of information about your specific case. They can tell you which tests they recommend and why.
There’s no way to cure either type of herpes simplex virus or varicella zoster virus, but it’s possible to manage and suppress the viruses. That keeps them from reactivating and causing a recurrent infection.
The main way to suppress these viruses is with antiviral medications. They interfere with how these viruses replicate (make more of themselves), which can treat a current infection or flare-up. And you can also take some of these drugs daily to prevent virus reactivation. Some drugs treat HSV or varicella specifically, while others can treat either.
These drugs can be intravenous (IV, through a vein), oral (pill), or topical eye drop or ointment forms. They include:
Your eye care specialist may also recommend other drugs to treat your infection or its symptoms. These often include:
People with more severe eye damage may need surgery.
Your eye care specialist can tell you:
Eye herpes can vary slightly depending on the virus that causes it and what part(s) of your eye it affects. It’s usually very painful, and it's common for it to cause other unpleasant symptoms like light sensitivity and watery eyes.
If you develop blisters or sores around your eyes or on your eyelids, see a healthcare provider or eye care specialist as soon as possible. Quick diagnosis and treatment are very important to avoid more serious eye complications.
If you have a child who has symptoms of ocular herpes, you should call or schedule an urgent appointment with their pediatrician. Eye herpes is the second-leading cause of cornea-related vision loss in children.
Ocular herpes isn’t life-threatening, but it can cause permanent vision loss and other issues. Fortunately, this condition is treatable and antiviral medications can reduce the risk of having recurrences. You’ll need to take these medications indefinitely because these viruses are a lifelong condition.
There’s no way to prevent eye herpes with 100% certainty. But there are several things you can do to significantly lower your risk of developing it, even if you catch one of the viruses that can cause it.
If you have eye herpes, it’s important to get it treated. The sooner you do, the less likely you are to have serious complications. You should also talk to a healthcare provider about taking antiviral medications to prevent the virus from reactivating and causing a recurrent infection.
If you have eye herpes, you may want to ask your eye care specialist or healthcare provider the following:
Eye herpes from HSV can have the following features:
Eye herpes from varicella zoster can look similar, but it can also have another distinctive feature: A rash, blisters or sores on one side of your forehead. That’s because the virus can spread through specific nerves in your forehead that branch very close to your eye.
Yes, viruses like HSV or varicella can spread through soiled cloth items, including pillow cases, towels, washcloths and others. Don’t share these items with someone who has HSV or shingles or if you have one of these infections. You should also wash towels and pillowcases daily and use separate washcloths for areas with an infection to reduce the chance of it spreading.
The viruses that cause eye herpes are common and spread in many ways. You might feel uncomfortable talking about herpes viruses with your provider, but your provider’s focus is on treating the condition so you can feel better. Early treatment can prevent serious complications and future recurrences. Don’t wait to reach out to an eye care specialist if you have symptoms of eye herpes or want to talk more about your risk of developing it down the road.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s ophthalmologists and optometrists have the highest training available. We provide exams, vision correction and care for many eye conditions.
