Gigantism is a very rare condition that happens when a child or adolescent has high levels of growth hormone in their body, which causes them to grow very tall. Gigantism is treatable, but early diagnosis is crucial to prevent excessive height and other complications.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
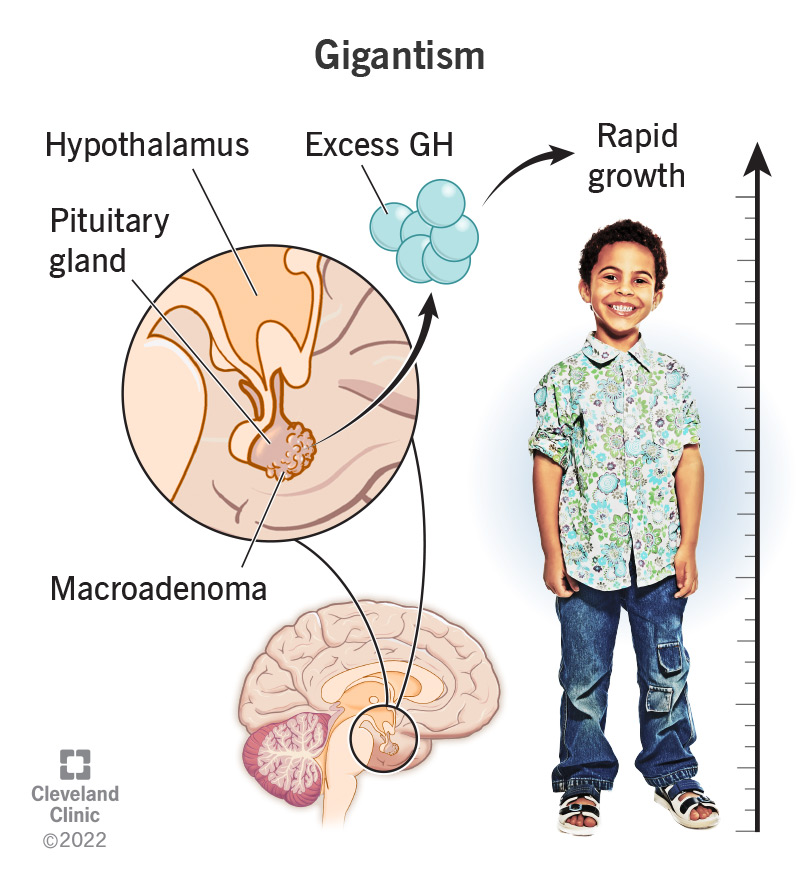
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/22954-gigantism)
Gigantism, also called pediatric acromegaly and pituitary gigantism, is a very rare condition that happens when a child or adolescent has high levels of growth hormone (GH) in their body, which causes them to grow very tall. The pituitary gland normally produces GH, but a tumor on their pituitary can produce excess GH in gigantism.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Your pituitary gland is a small, pea-sized endocrine gland located at the base of your brain below your hypothalamus. Your pituitary gland releases eight important hormones, including GH.
Growth hormone, also known as human growth hormone (hGH) and somatotropin, is a natural hormone that acts on many parts of the body to promote growth in children. Once the growth plates (epiphyses) in your bones have fused, GH no longer increases height. Instead, it helps to maintain normal bone, cartilage and organ structure and metabolism. GH is closely connected to insulin-like growth factor 1 (IGF1), a hormone your liver releases. These hormones work together to carry out growth and metabolism functions.
In gigantism, the excessive amount of growth hormone (GH) accelerates the growth of muscle, bones and connective tissue. This leads to an abnormally increased height as well as several soft tissue changes. When left untreated or unmanaged, some people with gigantism have grown over 8 feet tall.
Because of this, early diagnosis and treatment are crucial in cases of gigantism.
Gigantism and acromegaly are both conditions that result from excess growth hormone (GH). The difference is in who the conditions affect — adults develop acromegaly, whereas children and teenagers who are still growing develop gigantism.
Advertisement
In children, gigantism occurs when they experience excess GH before the growth plates in their bones fuse (before the end of puberty).
Once your growth plates have fused, excess GH causes acromegaly. In this case, you don’t grow in height, but the excess GH affects your bones’ shape and your organ size as well as other health factors.
Gigantism is rarer than acromegaly.
Though it’s very rare, gigantism can affect any child whose growth plates in their bones haven’t fused yet (they haven’t finished puberty). Gigantism commonly affects boys more than girls.
Gigantism is very rare. There’ve been approximately 100 cases recorded in the United States so far.
Growth hormone (GH) regulates growth during childhood by promoting measured bone, muscle and tissue growth and helping to control metabolism. Growth is normally a relatively stable process until a child reaches puberty.
During puberty, the release of sex hormones (estrogen and testosterone) increases significantly and causes the growth plates (epiphyses) at the ends of your child’s long bones to slowly fuse. Height growth stops at the end of puberty when the growth plates have completely joined.
The rate at which a child grows and their final height reached after puberty is determined by a combination of several genes they inherit from their parents, environmental factors and their sex.
In cases of gigantism, a child grows very rapidly and significantly more than other children of the same sex and age. But gigantism can still be difficult for parents to detect since symptoms of gigantism might seem like normal childhood growth spurts at first.
If you have any questions or concerns about the rate at which your child is growing, talk to their healthcare provider.
Excessive amounts of growth hormone (GH) cause the signs and symptoms of gigantism. Children with gigantism can also develop certain symptoms as their pituitary tumor applies pressure to their nearby brain and nerve tissues. The main sign of gigantism is excessive growth. Children with gigantism grow rapidly in height.
Aside from being very tall/large for their age, physical characteristics of gigantism include:
Other symptoms of gigantism include:
Advertisement
If your child experiences these symptoms, it’s important to talk to their healthcare provider as soon as possible.
The most common cause of gigantism is a benign (noncancerous) tumor on your child’s pituitary gland (a pituitary adenoma) that releases excess growth hormone (GH). Children with gigantism almost always have large pituitary tumors called macroadenomas (a pituitary adenoma that’s 10 millimeters in diameter or larger) at diagnosis. Gigantism can also be caused by pituitary hyperplasia, which is when your pituitary gland becomes enlarged.
Many children with gigantism have a genetic mutation that causes the pituitary tumor to form. The most common genetic mutations associated with gigantism are AIP gene mutations or deletions, making up approximately 29% of the population of people with gigantism.
Gigantism can occur as a part of several rare genetic disorders that lead to an increased risk of developing GH-secreting pituitary tumors, including:
Advertisement
Gigantism can be difficult to diagnose due to how rare it is and because growth rates can vary widely from child to child due to genetics and environmental factors.
In general, healthcare providers suspect gigantism when a child’s height is three standard deviations above the normal average height for their sex and age or two standard deviations above the adjusted average based on the height of their biological parents.
If your child’s healthcare provider thinks they may have gigantism, they’ll likely recommend you see an endocrinologist, a healthcare provider who specializes in hormone-related conditions. They’ll make a diagnosis based on your child’s medical and family history, a thorough clinical evaluation and specialized tests such as blood tests and imaging tests.
If your child’s healthcare provider suspects they have gigantism, they may order the following tests to help diagnose the condition:
Advertisement
If your child has been diagnosed with gigantism, their provider may order additional tests to see if the condition has affected other parts of their body. These tests may include:
The goals of treating gigantism include:
Healthcare providers typically use a combination of treatments, specifically surgery and radiation therapy, for gigantism.
Medications are available and effective in treating acromegaly (excess GH in adults) but the effects of these drugs on children haven’t been adequately studied.
Surgery is the most common treatment option for gigantism. The goal is to remove or reduce the size of the pituitary tumor. Since the pituitary tumors that cause gigantism are often large, children with gigantism may need multiple surgeries to remove the tumor and effectively regulate GH levels.
Your child’s surgeon may use a type of surgery called transsphenoidal surgery to remove the pituitary tumor, which involves going through your child’s nose and sphenoid sinus, a hollow space in your child’s skull behind the nasal passages and below your child’s brain, to perform surgery.
Radiation therapy can help lower growth hormone levels when surgery isn’t effective in doing so. Radiation therapy uses specialized equipment to target the tumor with radiation beams. This therapy works slowly. It may require several treatment courses, with breaks in between, and may take several years to fully take effect.
As a result of surgeries and/or radiation therapy, approximately 60% of people with gigantism develop hypopituitarism after treatment, a condition in which there’s a lack of one, multiple or all of the hormones made by your pituitary gland. Hypopituitarism is treated with hormone replacement medications.
Complications from surgery to remove a pituitary tumor can include:
Possible side effects of radiation therapy include:
The prognosis (outlook) for children and adolescents diagnosed with gigantism depends on several factors, including:
In general, people who are older at diagnosis tend to have more complications than people who are diagnosed at a younger age, probably due to longer exposure to excess growth hormone and insulin-like growth factor 1.
Because of this, it’s essential to talk to your child’s healthcare provider as soon as possible if you’re noticing abnormal or unexpected changes in their growth and/or physical features.
Early diagnosis and treatment of gigantism are crucial to prevent excessive height and associated complications and improve life expectancy.
If gigantism is left untreated, it’s associated with significant complications and an increased death rate of around twice the normal average.
Long-term complications that some people with gigantism might experience due to excessive height and the overall effects of excess growth hormone include:
Issues participating in everyday tasks such as buying clothes and traveling due to a very tall height can also diminish the quality of life of people with untreated gigantism.
Unfortunately, there’s nothing you can do to prevent gigantism, though early diagnosis is crucial. Prompt treatment can help prevent or slow the changes that cause your child to grow very tall.
If your child has been diagnosed with gigantism, they’ll need to see their healthcare provider and/or endocrinologist regularly to monitor treatment and to make sure their hormone levels are in an optimum range.
If you’re noticing changes in the rate at which your child is growing and/or changes in their physical features, it’s important to talk to their healthcare provider as soon as possible. While it may be unlikely that gigantism is the cause, any concerning changes are worth evaluating. People with gigantism who are diagnosed early have the best outlook and usually lead healthy lives. If you have any questions about what to expect with your child’s growth, don’t be afraid to reach out to their provider. They’re there to help.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.