Ovarian endometriomas, or “chocolate cysts,” are cysts filled with old blood. They’re a sign of endometriosis. These cysts can cause painful symptoms that your provider can help you manage. In some cases, removing them is the best option.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
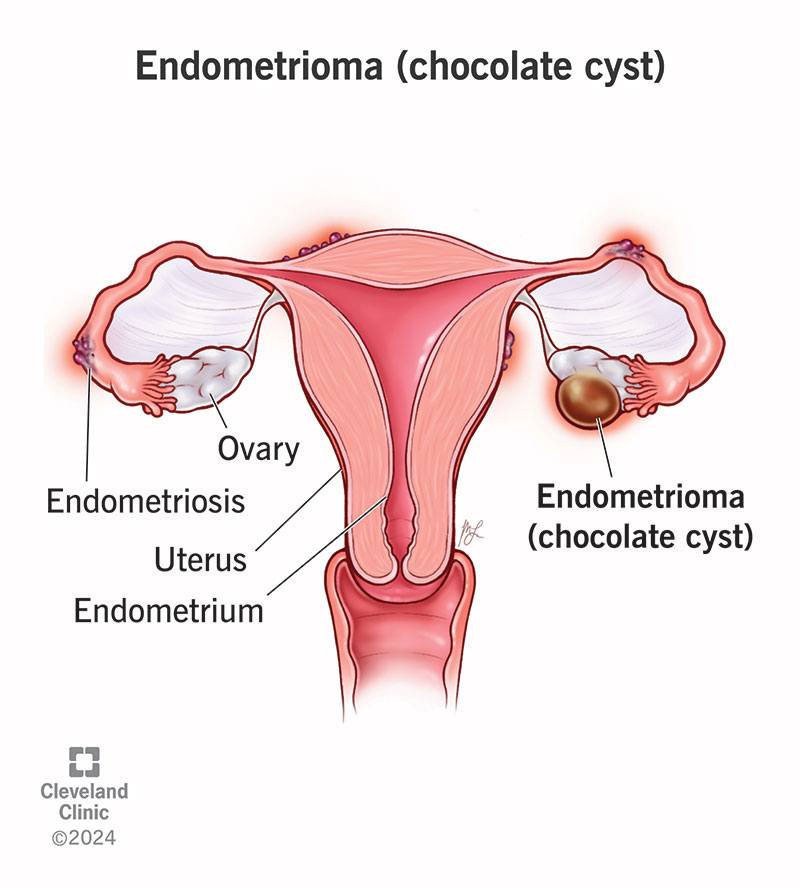
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/22004-ovarian-endometrioma)
An endometrioma is a type of cyst that forms on or inside your ovary. It’s usually filled with thick, brown fluid. It’s sometimes called a “chocolate cyst.” Endometriomas can be very small or grow large. They can affect one or both ovaries.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Endometriomas are associated with endometriosis, a condition where tissue similar to the lining of your uterus grows on other parts of your body. Endometriomas may be a sign of severe endometriosis.
Healthcare providers can treat endometriomas that cause pain, become large or affect fertility.
Studies estimate that between 17 and 44 in 100 women with endometriosis develop an ovarian endometrioma.
Pain or tenderness in your pelvis is the most common symptom. This pain can happen at any time, not just when you’re on your period. You may notice other symptoms, too, like:
One theory is that they form because some of the tissue-like lining that sheds during your period flows backward instead of leaving your body. This is called retrograde menstruation. The tissue can travel through your fallopian tubes and attach to your ovaries.
Over time, the tissue can thicken and bleed with each menstrual cycle. This may lead to irritation, inflammation and a cyst forming.
Endometriomas are cysts caused by endometriosis. Some of the factors that can raise your risk of endometriosis are:
Advertisement
In most cases, endometriomas are signs of a more advanced stage of endometriosis. Other than severe pelvic pain, some of the complications are:
Ovarian endometriomas can become cancerous, but this is rare. Your provider may monitor the cysts. They’ll discuss treatment options if there’s concern that it could become cancerous.
A pelvic exam and imaging tests can help diagnose an ovarian endometrioma. If the cyst is large, your provider may be able to feel it during a pelvic exam. A transvaginal ultrasound or MRI can help show the size and location of the cyst.
Sometimes, surgeons remove the cyst and send the tissue to a lab to confirm the diagnosis.
There isn’t a cure for ovarian endometriomas, but a surgeon can remove them if they cause symptoms or affect your health. Treatment options include:
The best treatment for you depends on lots of factors, like your age, your symptoms and your plans for becoming pregnant. Weigh the pros and cons of your options with your provider to decide the best option for you.
You don’t always have to remove an endometrioma. Small cysts that don’t cause pain may not need treatment.
Contact a healthcare provider if you have pelvic pain or other symptoms of an ovarian endometrioma. They can do an exam and order tests to see if an ovarian endometrioma is the source of your painful symptoms.
You should seek emergency care if you have an ovarian endometrioma that bursts. Pay attention to these warning signs:
Advertisement
Having ovarian endometriomas may be a sign of moderate to severe endometriosis. Your healthcare provider can work with you to help manage symptoms. They can also answer questions about fertility if you’re trying to get pregnant.
Yes, you can. It may be more difficult depending on the size of the endometrioma or if it affects both ovaries. Your healthcare provider can give you more information based on your situation.
Yes, they can come back after treatment. The risk depends on the size of the cyst, your age and the type of treatment.
If you have endometriosis, then you know that it can be very painful and disruptive to your life. Developing an ovarian endometrioma on top of that can be even more upsetting. And knowing that painful symptoms usually get better after menopause isn’t always comforting, especially if you’re trying to start a family. If you have an endometrioma, talk to your provider about the treatment options available to you. They can recommend ways to help you feel better.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Endometriosis symptoms can interrupt your life. At Cleveland Clinic, our experts create a treatment plan that matches your lifestyle and goals.
