Thyroid cancer develops in your thyroid gland, a part of your endocrine system. Your thyroid gland produces hormones that regulate body temperature, heart rate and metabolism. Most thyroid cancers are curable. Treatments include surgery, radioiodine therapy and targeted therapy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
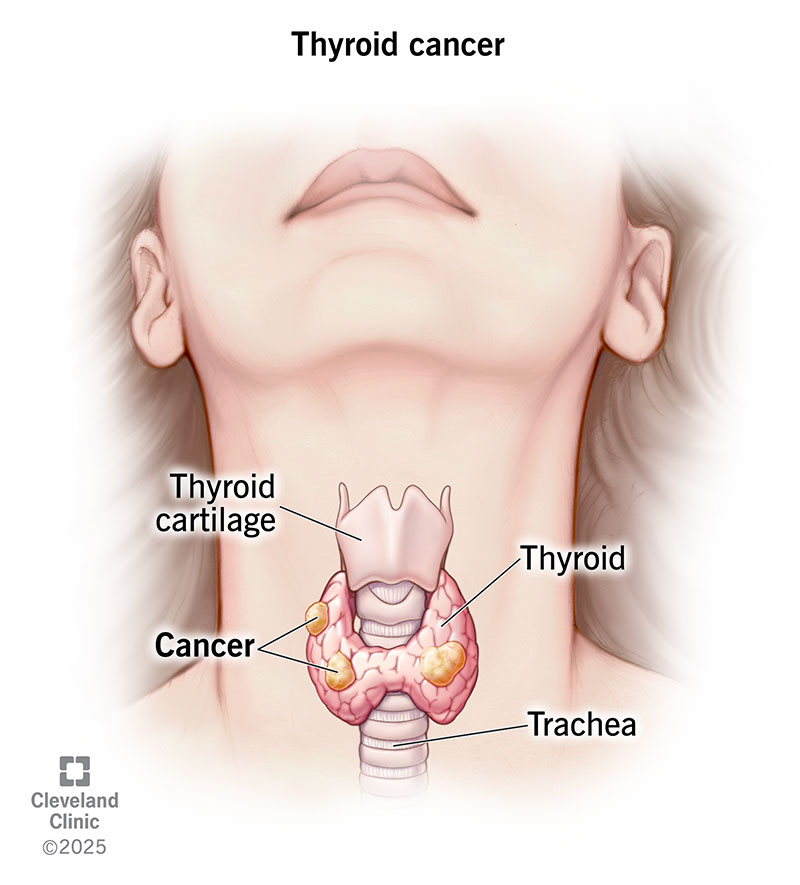
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/Images/org/health/articles/12210-thryoid-cancer)
Thyroid cancer develops in your thyroid, a small, butterfly-shaped gland at the base of your neck. This gland makes hormones that regulate how your body uses energy. Thyroid hormones also help control your body temperature, blood pressure and heart rate.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
About 44,000 people in the U.S. develop cancer in their thyroid glands each year. Most are treatable and curable.
But your experience depends on lots of things, like the type of thyroid cancer and how advanced it is.
Healthcare providers classify thyroid cancer based on the type of cells from which the cancer grows. The most common types of thyroid cancer include:
Advertisement
The first sign of thyroid cancer is usually a painless lump in your neck. It’s called a thyroid nodule. But don’t panic if you feel one. Most nodules aren’t cancer. Only about 1 out of 10 thyroid nodules turns out to be cancerous.
Most thyroid cancers don’t cause any symptoms. Your healthcare provider may find it during an unrelated procedure.
Some symptoms associated with thyroid cancer include:
Thyroid cancer forms when DNA in a cell changes (mutates). Most mutations happen over time, but some are passed down from your biological parents.
Females are three times more likely than males to get thyroid cancer. It’s more common in females in their 40s and 50s, and males in their 60s and 70s.
Other risk factors include:
If you have signs of thyroid cancer, your healthcare provider may order one or more of these tests:
Thyroid cancer stages range from 1 (I) to 4 (IV). The higher the number, the bigger the tumor or the more the cancer has spread. Usually, cancer cells spread to nearby structures and lymph nodes first. After that, they spread to distant lymph nodes, organs and bones.
The specifics of thyroid cancer staging systems differ based on the cancer type. Your age matters, too, for some thyroid cancer types. To learn how cancer staging applies to you, talk to your healthcare provider.
Surgery is the most common treatment. A surgeon may remove all of your thyroid gland (thyroidectomy). Or they may just remove the diseased parts (lobectomy). They’ll also remove any lymph nodes where cancer cells are.
Other treatments include:
Advertisement
If you have surgery or radiation to your thyroid, you’ll likely need thyroid hormone replacement therapy for life. You may get synthetic thyroid hormones, like levothyroxine (Synthroid®).
You’ll need regular doctor visits so your provider can see if the cancer has come back after treatment. Thyroid cancer can return, but it’s uncommon. Only 2 out of 10 papillary thyroid cancers (the most common type) recur.
Call your healthcare provider if you notice signs that the cancer has come back after treatment. Usually, blood work detects signs of recurrence. But you may notice new neck swelling or enlarged lymph nodes.
Thyroid cancer has a five-year survival rate of over 98%. This means that you’re about just as likely to live for at least five years as someone who doesn’t have thyroid cancer. Usually, the cancer stays in remission. Remission means there are no signs or symptoms of cancer.
These numbers vary, though, depending on the cancer type and cancer stage. For example, the five-year survival rate is excellent even when papillary and follicular cancers have spread. On the other hand, less than half of people with advanced medullary thyroid cancer survive. All forms of the rare anaplastic type involve a shortened life expectancy.
Advertisement
Your healthcare provider can explain how your diagnosis relates to your life expectancy.
Yes, most thyroid cancers are permanently curable with treatment. This is especially the case if the cancer hasn’t spread to distant parts of your body. Treating thyroid cancer in the early stages reduces the risk of cancer spread.
If treatment doesn’t fully cure thyroid cancer, your healthcare provider can design a treatment plan to manage it.
Not usually. But if you know you’re at risk, you may be able to take steps for early detection. Options include:
Anyone can get thyroid cancer. But the average age of diagnosis is 51. Females tend to get diagnosed at younger ages than males.
Thyroid cancer is the second most common cancer diagnosed in pregnancy. Breast cancer is the first.
Advertisement
Your healthcare provider may delay treatment until after you deliver your baby. If treatment can’t wait, most people can safely have surgery to remove the cancerous gland. Your provider may wait to use tests or treatments involving radiation until after you’ve finished breastfeeding.
Receiving a cancer diagnosis is unsettling, regardless of the type. Fortunately, most thyroid cancers respond well to treatment. Your healthcare provider can discuss the best treatment option for the type of thyroid cancer you have. After treatment, you may need to take thyroid hormones for life. These hormones support vital body functions. You’ll also need regular checkups to monitor your health.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Hearing you have cancer can be scary. But most thyroid cancer is treatable, and the providers at Cleveland Clinic are here to help.
