Myasthenia gravis affects how your nerves communicate with your muscles. It leads to muscle weakness that worsens throughout the day and with activity. Drooping eyelids and/or double vision are often the first sign. You may find it difficult to stand, lift objects and speak or swallow. Medications and surgery can help relieve the symptoms of this lifelong illness.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Myasthenia gravis is an autoimmune condition that causes skeletal muscle weakness. These are the muscles that connect to your bones and help you move. Myasthenia gravis usually targets the muscles in your eyes, face, neck, arms and legs. It can affect your ability to:
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Muscle weakness gets worse after physical activity and improves after rest. Symptoms usually happen quickly.
Myasthenia gravis is a chronic (long-lasting) neuromuscular condition (it affects the junction between your nerves and muscles). There isn’t a cure, but effective treatment can help you manage your symptoms and function well.
The types of myasthenia gravis include:
There are two subtypes of autoimmune myasthenia:
Advertisement
Myasthenia gravis affects about 20 out of every 100,000 people around the world. The actual number may be higher, as some people with mild cases may not know they have the condition. In the United States, there are approximately 60,000 people affected by myasthenia gravis at any given time.
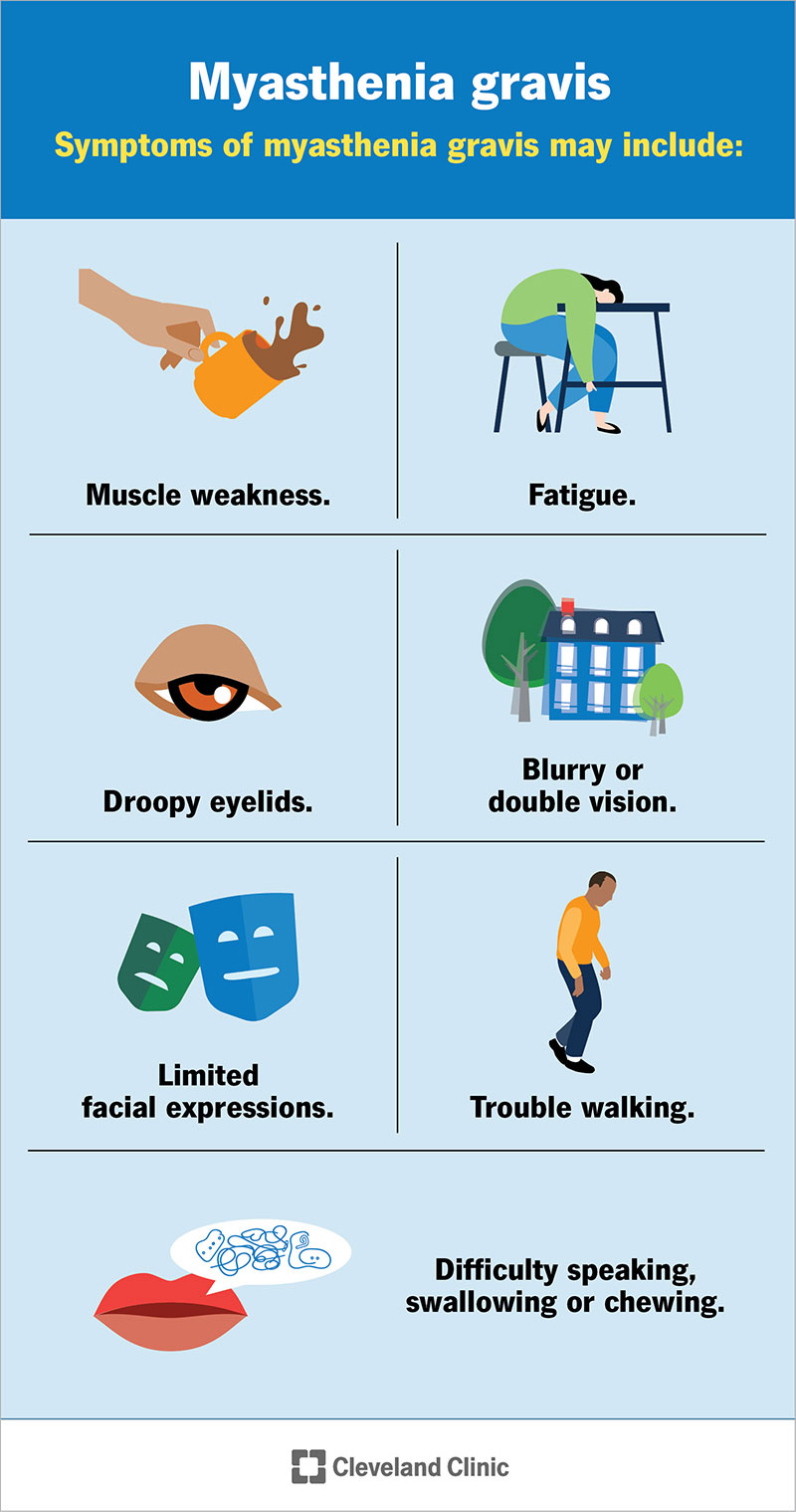
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/17252-myasthenia-gravis-mg)
Symptoms of myasthenia gravis may include:
Initial symptoms of myasthenia gravis happen suddenly. Your muscles usually get weaker when you’re active. Muscle strength returns when you rest. The intensity of muscle weakness often changes from day to day. Most people feel strongest at the start of the day and weakest at the end of the day.
In rare instances, myasthenia gravis affects muscles in your respiratory system. You may have shortness of breath or more serious breathing problems. Contact 911 or your local emergency services number if you have trouble breathing. In general, this doesn’t occur suddenly.
Myasthenia gravis (autoimmune type) happens when your body’s immune system mistakenly attacks itself. Researchers aren’t sure why this happens. Studies suggest that certain immune system cells in your thymus gland have trouble identifying what’s a threat to your body (like bacteria or viruses) versus healthy components.
A genetic change causes congenital myasthenia. Antibodies passed from a birth mother to a fetus during pregnancy cause neonatal myasthenia.
Myasthenia gravis affects communication between nerves and muscles.
When your immune system is working as expected, nerves and muscles work together. It’s similar to a baseball game:
If you have myasthenia gravis, antibodies destroy the receptor sites, blocking nerve-muscle communication. The “catcher” can’t catch the ball, and communication becomes sluggish or doesn’t work at all.
It’s rare to inherit autoimmune myasthenia gravis. You can inherit congenital myasthenia or neonatal myasthenia. Types where inheritance happens usually occur in an autosomal recessive pattern where you need two genes, one from each biological parent, to experience symptoms.
Advertisement
Myasthenia gravis is most common among females around age 40 and males after age 60. The condition can affect anyone at any age.
You may be more at risk of developing myasthenia gravis if you:
If you have myasthenia gravis, your symptoms could trigger (start) if you:
Weakness and fatigue from myasthenia gravis can keep you from participating in activities you enjoy. This may lead to stress and depression. However, studies also show that most people with myasthenia gravis can tolerate light activities and exercises on a routine basis.
Up to 1 in 5 people with myasthenia gravis experience a myasthenic crisis or severe respiratory muscle weakness. You may need a respirator or other treatments to help you breathe. This is a life-threatening medical emergency. An estimated 20% of people with myasthenia gravis experience at least one myasthenic crisis in their lifetime.
Many people with myasthenia gravis have thymus gland conditions that may trigger symptoms. The thymus is a small organ in your upper chest. It’s part of your lymphatic system. It makes white blood cells that fight infections. Two-thirds of people with myasthenia gravis have overactive thymic cells (thymic hyperplasia). About 1 in 10 people with myasthenia gravis have thymus gland tumors called thymomas, which may be benign (not cancer) or cancerous.
Advertisement
To diagnose myasthenia gravis, your healthcare provider will perform a physical exam and ask detailed questions to learn more about your symptoms and medical history. Testing confirms a diagnosis. It may include:
There are five main classifications of myasthenia gravis that your healthcare provider may use during a diagnosis:
There’s no cure for myasthenia gravis. But effective treatment is available to help manage your symptoms. Treatments may include:
Advertisement
Common medications to treat myasthenia gravis include:
Side effects are possible with these medications. Talk to your healthcare provider to learn more before starting a new medication.
If you have myasthenia gravis, try these steps to ease fatigue and boost muscle strength:
Myasthenia gravis is a treatable condition. Symptoms range from mild to severe. Symptoms tend to reach their peak in severity within one to three years of initial diagnosis.
Most people with the condition live full and active lives with treatment.
Some cases go into remission. Remission is when your symptoms stop for a period of time. This could be temporary or permanent. If remission happens, your healthcare provider may adjust your treatment plan.
Most people have a normal life expectancy with myasthenia gravis. Life-threatening outcomes may happen during a myasthenic crisis, which affects your ability to breathe.
In rare instances, pregnancy brings on myasthenia gravis symptoms for the first time. If you already have this condition, symptoms may worsen during the first trimester or immediately after childbirth. In some cases, myasthenia gravis symptoms improve during pregnancy.
Certain treatments aren’t safe during pregnancy or breastfeeding. Your healthcare provider can guide you through this time, ensuring a healthy pregnancy.
You should call your healthcare provider if you experience:
Call 911 or your local emergency services number if you have trouble breathing.
You may want to ask your healthcare provider:
It’s challenging to live with a chronic illness like myasthenia gravis. When you want to be active, you might feel too tired or weak to participate. This can take a toll on your mental and physical health over time. Although there isn’t a cure, most people with this condition lead full and active lives with treatment. Severe disabilities from myasthenia gravis are extremely rare. Your healthcare provider can suggest ways to manage symptoms so you can feel better.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic can provide you with the latest, personalized treatment for myasthenia gravis so that you can do what you love.
