Adjuvant therapy is treatment you may have after cancer surgery to remove a tumor. It’s a common treatment for several cancer types, including breast cancer and lung cancer. Adjuvant therapy may involve systemic therapies, like chemotherapy, targeted therapy or hormone therapy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
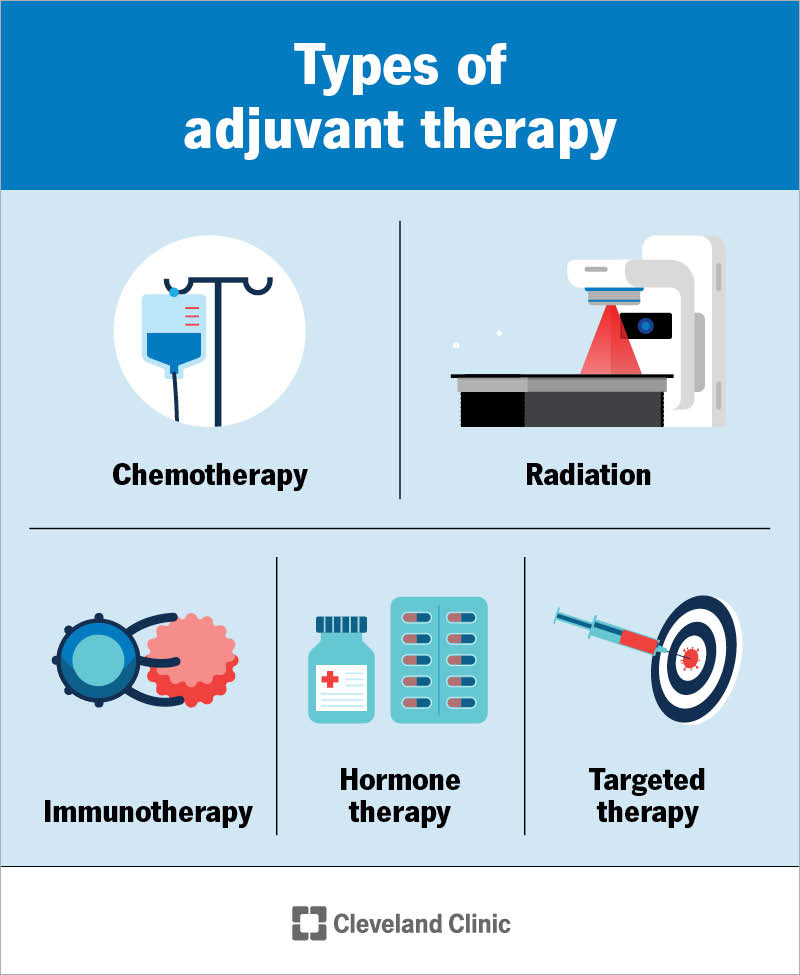
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/22483-adjuvant-therapy)
Adjuvant therapy is treatment after cancer surgery to destroy tiny cancer cells that surgery misses. It’s also known as helper therapy. Adjuvant therapy may reduce the risk that cancer will come back or spread. It may also help you live longer. People with breast cancer, colorectal cancer, non-small cell lung cancer or melanoma may have adjuvant therapy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Your surgeon may recommend this treatment even if surgery has removed a tumor. They base their recommendation on factors like:
Adjuvant therapy typically involves systemic therapies, like:
Advertisement
Your provider may use radiation therapy as adjuvant therapy for breast cancer and lung cancer. The treatment targets the areas where cancer was first found.
Research shows adjuvant therapy may keep cancer from coming back. Success rates differ based on factors like cancer type, stage and the specific medications used in adjuvant therapy.
Researchers continue to study the impact of adjuvant therapy. For example, one study found that half of the people with stage III melanoma were cancer-free seven years after adjuvant therapy. Another recent study found that, in some cases, about 9 out of 10 children who had radiation therapy after surgery to remove a brain tumor were alive five years after treatment. And immunotherapy is an effective adjuvant treatment for non-small cell lung cancer and other cancer types.
Ask your cancer care team about cancer rehabilitation and palliative care. With cancer rehabilitation, specialists help you get ready for adjuvant therapy. For example, some cancer treatments affect your appetite. A nutritionist will suggest ways to get the nutrition you need. A physical therapist may recommend gentle exercise to help you manage fatigue and stress.
Palliative care is holistic treatment and support. Specialists can help you manage treatment side effects. They can also connect you with mental health support, community programs and spiritual support.
Talk to your cancer care team if you have treatment side effects that are stronger than you expect or you need help managing side effects. There are many things your team can do to ease these effects. Your team will move quickly to help you.
Both treatments help make cancer surgery more effective. Neoadjuvant therapy is cancer treatment before surgery. The treatment, often chemotherapy, immunotherapy or radiation therapy, may help shrink a tumor so it’s easier to remove. Adjuvant therapy targets microscopic cancer cells that surgery may miss.
Cancer treatment may feel like a series of hurdles: You have to leap each one to get to the finish line and be free of cancer. Adjuvant therapy may feel like an unexpected additional hurdle that slows you down when the finish line is in sight. But cancer is a challenging disease, in part because microscopic cancer cells can duck detection.
It can be frustrating to learn that, after all you’ve done to be finished with cancer, there’s still a chance it can come back. Your cancer care team will understand. They’ll take time to explain how adjuvant therapy may make a difference. They’ll also discuss the side effects of treatment and how they’ll help you manage them.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
When you’re diagnosed with cancer, you want expert and compassionate care right away. At Cleveland Clinic we personalize your treatment to match your needs.
