You might need to have a cholecystectomy, surgery to remove your gallbladder, if you have a chronic or persistent gallbladder disease. Gallstones are the most common reason. If you have this surgery, you’ll be in good company. It’s one of the most common procedures performed worldwide. In the U.S., most surgeons offer it as a laparoscopic procedure.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
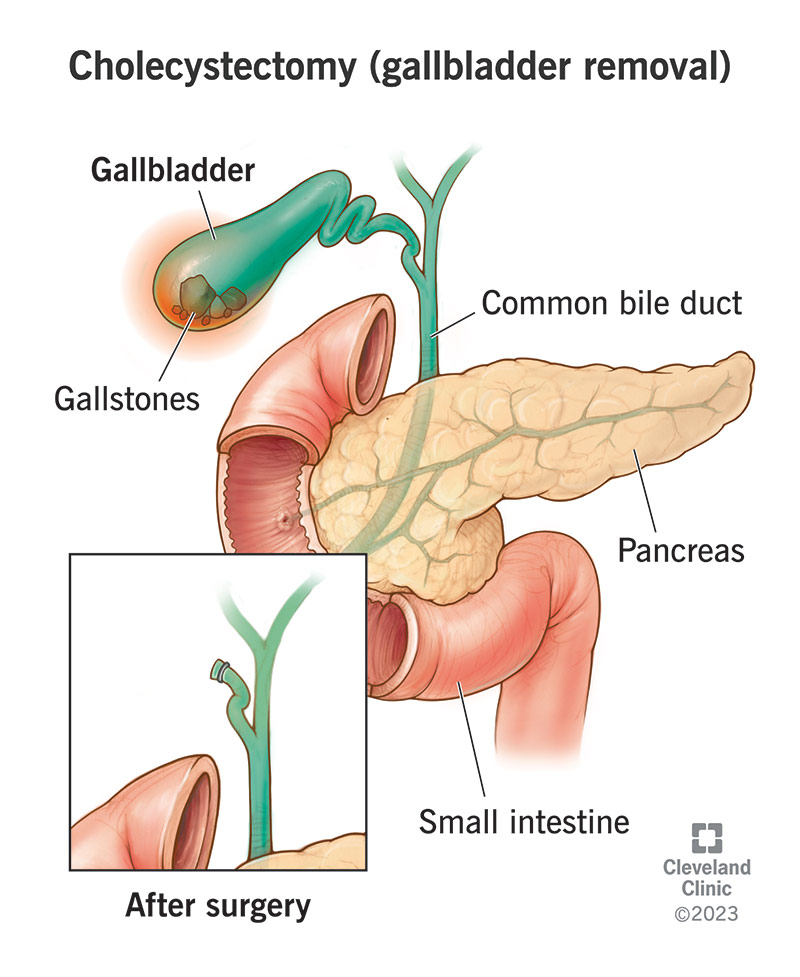
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/Images/org/health/articles/cholecystectomy-gallbladder-removal)
A cholecystectomy is a surgical operation to remove your gallbladder — the small, hollow organ that stores bile for your digestive system. Gallbladder removal surgery is a common treatment for gallbladder disease because these conditions often cause more problems than the surgery. You can live a healthy life without a gallbladder.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Gallstones are the most common reason for a cholecystectomy. Some people have no symptoms, but those who do often have repeat issues.
You might need gallbladder removal surgery if gallbladder disease:
That’s often true for conditions like:
Gallbladder removal changes how bile flows in your body. Instead of storing extra bile for digestion, your liver sends it straight to your small intestine.
Most people experience a temporary adjustment period in their digestive systems after gallbladder removal. For the first month or so, you might have more trouble digesting fats and heavier meals. This should gradually improve over time.
Most people can resume a normal, healthy eating plan after their recovery. But a small number of people develop longer-term digestive difficulties, for unclear reasons.
Cholecystectomy is a common procedure with a relatively easy recovery. Surgeons do most laparoscopically, using small incisions to reduce pain and speed healing. Sometimes, people need open surgery, but laparoscopic is the standard.
To get you ready for surgery, your care team will:
Advertisement
When it’s time, you’ll get an IV for fluids and medicine. You’ll go under general anesthesia. A breathing tube will help keep your airway open during surgery.
Laparoscopic surgery:
Your surgeon will:
Open surgery:
Your surgeon will:
A laparoscopic cholecystectomy normally takes about 60 to 90 minutes. An open cholecystectomy takes about one to two hours. It may take longer if your surgeon also checks or clears your bile ducts during surgery.
Most gallstones develop inside your gallbladder, so removing your gallbladder significantly reduces the chance that you’ll have any more. If gallstones have brought you to the hospital once, they’re likely to do so again. Cholecystectomy is the only treatment that can reliably prevent this. Most people feel it’s easier to have a planned procedure than to expect to have repeat episodes of gallstone emergencies.
There’s always a small risk of complications during surgery.
Specific risks of cholecystectomy include:
After surgery, you’ll spend a few hours in a recovery room while you wake up from the anesthesia. You’ll have pain medication as needed. If you had a laparoscopic cholecystectomy, you might be able to go home the same day. If you had an open cholecystectomy, you’ll need to spend a few days recovering in the hospital. Your drain may remain in place for a few days. In some cases, you might go home with it.
The recovery time from a laparoscopic cholecystectomy is about two weeks. Recovery from an open cholecystectomy takes six to eight weeks. If you still have a drain in your wound, your healthcare team will remove it at your next appointment. Most people can return to work after one to two weeks. But if you do a lot of physical activity, you might need to modify your routine until you’re fully recovered.
Advertisement
You may need to adjust your diet after gallbladder removal. Surgery and anesthesia can affect your digestive system, and your body will need time to adapt to the change in how it gets bile. Start with simple, bland foods — similar to what you’d eat if you had the flu. You may have trouble digesting high-fiber or high-fat foods at first. Your provider will guide you as you return to a normal, healthy eating pattern.
Most people have only short-term side effects during their recovery from cholecystectomy surgery. These might include:
Your healthcare provider can offer advice on how to manage these short-term conditions.
A small percentage of people experience longer-lasting symptoms after a cholecystectomy. Healthcare providers refer to this as post-cholecystectomy syndrome. But these symptoms, and their possible causes, are wide-ranging and don’t really describe one single condition. Post-cholecystectomy syndrome is usually a temporary diagnosis. It stands in until a provider can make a more specific one.
Advertisement
Symptoms can include:
Most people have one or a few of these symptoms, but not all.
Possible contributing causes include:
Healthcare providers treat these symptoms and conditions on a case-by-case basis.
Your healthcare provider will schedule a follow-up appointment with you a few weeks after your surgery. But be sure to contact them sooner if you develop symptoms of illness, like:
Thousands of people have successful cholecystectomies each year; most without any complications or side effects. Minimally invasive surgery techniques make recovery easier than ever before. Healthcare providers continue to recommend it as an elective procedure to treat persistent gallbladder diseases, like gallstones. These diseases pose a much higher risk to your health than gallbladder removal does.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
If you have issues with your digestive system, you need a team of experts you can trust. Our gastroenterology specialists at Cleveland Clinic can help.
