Ductal carcinoma in situ (DCIS) is cancer in your breasts’ milk ducts. It isn’t aggressive and it typically doesn’t spread. This early form of breast cancer is usually curable with appropriate treatment, which often includes lumpectomy and radiation therapy. DCIS is highly treatable, and the outlook is excellent.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
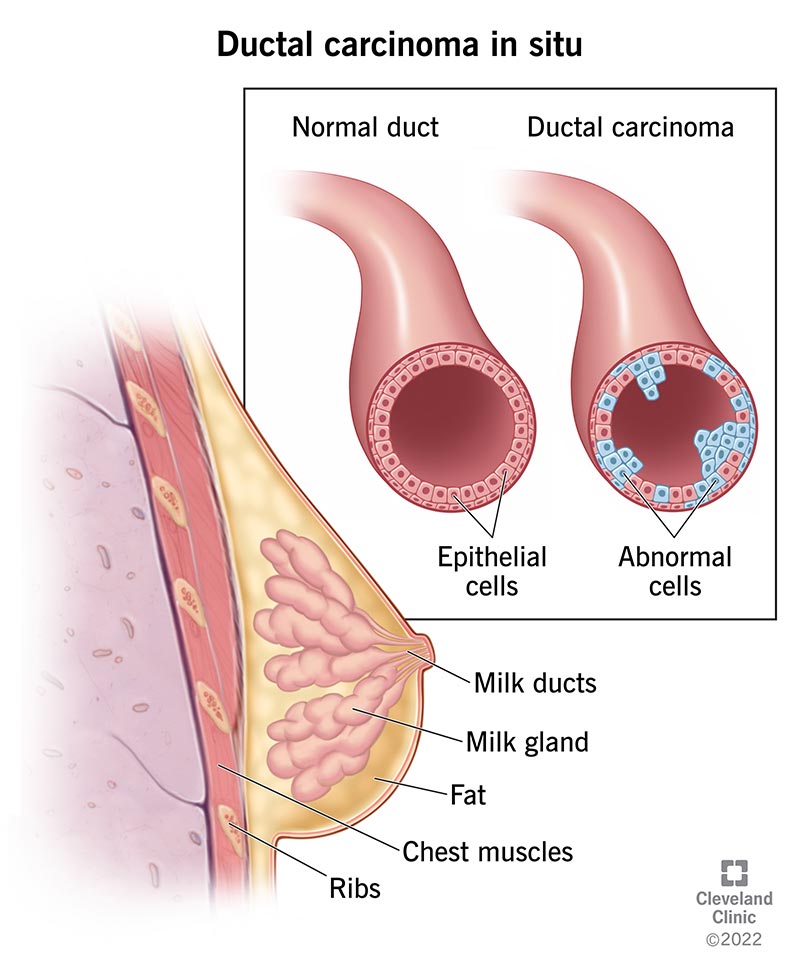
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/Images/org/health/articles/17869-ductal-carcinoma)
Ductal carcinoma in situ (DCIS) is a type of very early breast cancer where cancer cells line your milk ducts within one or both breasts. Milk ducts are tubes that carry milk from the lobes of your breasts to your nipples so you can breastfeed. The cancer is “in situ,” or situated (contained) inside of your milk ducts.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Healthcare providers may call DCIS noninvasive or pre-invasive breast cancer. This means that the cancer cells haven’t spread beyond the walls of your milk ducts. Ductal carcinoma in situ doesn’t typically metastasize, or spread to other organs in your body, as aggressive or invasive cancers do.
While DCIS can’t spread outside of your breast, it can turn into invasive ductal carcinoma — which can spread outside of your breast — in some cases. That’s why talking to a healthcare provider is so important. They can discuss treatment options to help reduce this risk.
Ductal carcinoma in situ is a common form of breast cancer among women, accounting for 20% to 25% of new breast cancer diagnoses each year. Men can get DCIS, but it’s rare (less than 0.1% of cancer diagnoses).
DCIS cases are on the rise. But experts believe this is because more people are being diagnosed and treated, not because more people are getting DCIS.
Ductal carcinoma in situ doesn’t generally cause symptoms. But a few people with DCIS may notice a breast lump, itchy skin or nipple discharge (like blood).
DCIS happens when healthy cells in your milk duct mutate (change) and grow uncontrollably. But experts aren’t sure why these changes take place to begin with, or why DCIS spreads in some cases but not others.
Advertisement
Certain factors can increase your risk of ductal carcinoma in situ, like:
Having a risk factor doesn’t mean you’ll get DCIS. For example, although a family history of breast cancer is a risk factor for DCIS, most people with ductal carcinoma in situ don’t have family members with breast cancer. Risk factors are all about probability — what may increase your chance of developing a condition.
Ductal carcinoma in situ can turn into invasive ductal carcinoma if you don’t treat it. If you have DCIS, it’s important to get treatment as soon as possible.
If you’ve received treatment for DCIS, you have a higher risk of developing other health conditions as you age. This includes osteoporosis, high blood pressure and heart disease. To reduce your risk of these complications, ask your healthcare provider how often you should have screenings and follow-ups.
Healthcare providers detect over 90% of DCIS cases during mammograms. If you receive suspicious mammogram results, they’ll do a biopsy.
Healthcare providers categorize DCIS into three grades:
Ductal carcinoma in situ is a highly treatable and curable stage 0 breast cancer. Healthcare providers classify cancer into stages from 0 to IV (4). Although DCIS is always stage 0, the tumor can be any size and may be located within several milk ducts inside of your breast.
Although DCIS isn’t an aggressive cancer, it’s still important to get treatment or have a healthcare provider monitor your condition closely. Some forms of ductal carcinoma in situ may become invasive without treatment. This means that the cancer spreads beyond your milk ducts and into your surrounding breast tissue.
Advertisement
The most common treatments for DCIS are breast-conserving surgery (lumpectomy) with radiation or a mastectomy:
Breast reconstruction may be an option if you’ve had a mastectomy. If you have BCS, you likely won’t need breast reconstruction. Speak with your healthcare provider about your preferences for how you’d like your breasts (chest) to look after treatment.
After surgery, your healthcare provider may prescribe medications to prevent DCIS from recurring (coming back). The most common medicines are tamoxifen (Nolvadex®) and aromatase inhibitors (like anastrozole). This treatment is called hormone therapy. The whole treatment course lasts for five years.
Advertisement
DCIS survival rates are excellent. According to the American Cancer Society, nearly all people with ductal carcinoma in situ can be cured with treatment.
After treatment, outcomes are usually excellent. Ductal carcinoma in situ rarely recurs (returns). Even in those instances where DCIS does recur, the cancer isn’t life-threatening.
Many of the risk factors for DCIS aren’t preventable. Still, you can improve your chance of curing DCIS by catching it early. Most women should start receiving yearly mammograms at age 40.
Talk to your provider about how often you should get a mammogram based on your risk factors.
With DCIS, expect to see your healthcare provider for a physical exam every six to 12 months for five years after treatment and then, annually. You’ll also likely need to get annual mammograms.
Still, everyone’s case is different. Work with your provider to determine your care plan following treatment.
Follow your healthcare provider’s guidance so you receive check-ups and mammograms as frequently as you should. In the meantime, pay attention to your breasts so you don’t miss signs of breast cancer.
If you have DCIS, here are some questions you may want to ask your healthcare provider:
Advertisement
Hearing that you have cancer is a life-changing event. There are so many unknowns, it’s natural to feel scared or worried. Your healthcare provider is here for you. Ductal carcinoma in situ (DCIS) is one of the most treatable cancers, and your provider can design a personalized plan for you.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
A breast cancer diagnosis can turn your world upside down. At Cleveland Clinic, we offer expertise, compassion and personalized treatment plans.
