What is tetralogy of fallot?
Tetralogy of Fallot (teh-TRALL-uh-jee of fuh-LOW) is a complex problem that involves four heart defects. The condition is congenital, which means it is present at birth. It affects about 5 out of every 10,000 babies.
TOF and blood flow
The defects involved in TOF affect blood flow and cause an oxygen crisis in the body. Normally, oxygen-poor blood flows from the top right chamber of your heart (atrium) to the bottom right chamber (ventricle). From there, it goes through the pulmonary artery to the lungs, where it gets oxygen. The oxygen-rich blood travels through the pulmonary vein into the left atrium, and then into the left ventricle. The blood flows out of the left ventricle into the aorta and out to the rest of your body.
There are four valves in your heart that control the direction of blood flow. Flaps (leaflets) inside the valves open and close to keep blood from flowing backwards.
A wall made of tissue (septum) divides the left and right sides of the heart.
TOF defects
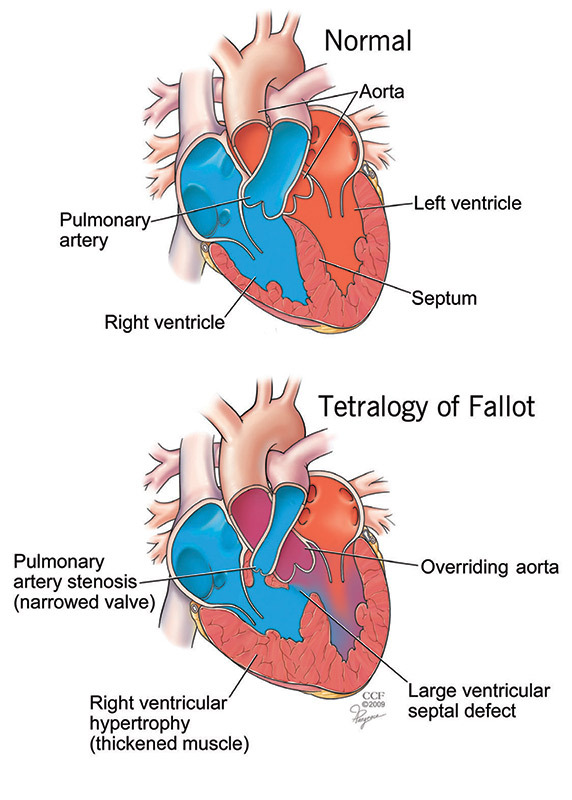
- Ventricular septal defect (VSD): A hole in the area of the septum that separates the left and right ventricles. The hole lets oxygen-poor blood from the right side mix with oxygen-rich blood in the left side. The mixed blood, which is low in oxygen, goes out to the rest of the body. This can cause your skin, nails, lips and the area around your eyes turn blue/gray (cyanosis).
- Pulmonary stenosis: The valve between the right ventricle and the pulmonary artery is narrowed. The narrowing often involves the valve and the muscle directly below it. Because the passageway to the pulmonary artery is narrow, your heart has to work harder to pump out the blood, and less blood is able to flow through the valve.
- Right ventricular hypertrophy: The muscle in your right ventricle is thicker than normal. This is caused by the extra work your heart needs to do because of pulmonary stenosis.
- Overriding aorta: The aorta is your body’s main artery. The aorta is normally connected to the left ventricle. If you have TOF, the aorta is attached to your heart between the left and right ventricles, above the ventricular septal defect. Because of this, blood flows into the aorta from both sides of the heart, and oxygen-poor blood from the right ventricle mixes with oxygen-rich blood from the left ventricle.
What causes TOF?
Tetralogy of Fallot was discovered more than 130 years ago, but the exact cause of the condition is still unknown.
The defects develop during pregnancy. Risk factors related to pregnancy include:
- Mother is over age 40.
- Poor nutrition.
- Alcohol use.
- Viral infection or diabetes.
About 15% of people with TOF have a specific genetic abnormality that is linked to other birth defects, such as cleft palate.
How is TOF diagnosed?
Tetralogy of Fallot often causes cyanosis that gets progressively worse during the first few weeks of life. So, a diagnosis is made very early in life. But sometimes it takes a few months or even several years for a person to be diagnosed with the condition.
Surgery to correct TOF
Surgery is needed to correct the problems related to TOF. The repairs are sometimes done in stages. This approach involves surgery within the first few weeks of life to place a shunt that increases blood flow to the lungs. This palliative surgery can help control symptoms until childhood. Then, surgery is done to fix the other problems.
Patients who have palliative surgery for TOF need regular follow-up care with a cardiologist.
Thorough evaluations are needed to check for problems like narrowing of the shunt, high blood pressure in the pulmonary arteries, too much blood flow to the left side of the heart or abnormal blood vessels that form to increase blood flow to the lungs.
A complete repair involves closing the VSD with a patch, repairing or replacing the pulmonary valve, and improving blood flow through the right ventricle and pulmonary arteries.
Complete repair surgery can cause problems such as:
Electrical disturbances: The patch used to fix the VSD can block electrical signals from the atria to the ventricles (heart block). This problem can be fixed with a pacemaker.
Abnormal heart rhythms (arrhythmias):
- Atrial fibrillation: A fast, irregular rhythm in the atria that keeps blood from flowing into the ventricles like it should. The problem is corrected with medicine or a nonsurgical procedure.
- Ventricular tachycardia: A rare, life-threatening fast rhythm that starts in the ventricles. The problem is corrected with medicine, a nonsurgical procedure or implantable cardioverter defibrillator.
Your surgeon will assess your risk of arrhythmias before you have surgery.
Leaky valve: Heart valves are designed to let blood flow in only one direction. Sometimes, a valve can leak, letting blood flow backwards. The most common valve problem after complete repair surgery for TOF is a leaky pulmonary valve. The problem is corrected by replacing or repairing the valve.
Residual VSD: Sometimes there is leakage around the VSD patch. If the leak is large or causes major symptoms, surgery is used to correct the problem.
Aneurysms: The VSD patch can cause weak sections of the ventricle to bulge out and form an aneurysm. Patients with TOF are also at risk of having aneurysms in the ascending aorta. Aneurysms need to be watched by a vascular specialist, and surgery is needed once it reaches a certain size.
Follow-up care after complete repair surgery for TOF
Adults who have complete repair surgery for TOF need regular follow-up visits with an adult congenital heart disease specialist. You may need an echocardiogram, Holter monitoring, electrocardiogram or exercise stress test to make sure your heart is working as it should.
Restrictions: Your doctor will talk to you about long-term restrictions after your surgery, such as not taking part in strenuous activities like competitive sports.
Pregnancy: Women who are considering pregnancy after complete repair surgery should talk to an adult congenital heart disease specialist and an obstetrician who specializes in high-risk pregnancy. They can help assess the risks of pregnancy. With proper prenatal care and careful monitoring, most women are able to have full-term pregnancies after surgery.
For more information
- Adult Congenital Heart Association, achaheart.org, 888.921.ACHA.
- American Heart Association, heart.org, 800.242.8721.
- International Society for Adult Congenital Cardiac Disease, isachd.org, 919.861.5578.
