Overview of percutaneous treatment options for patients with mitral valve disease
Cleveland Clinic cardiologists and surgeons work together to offer patients a variety of procedures and devices to repair and replace the mitral valve. Patients with mitral valve disease who are too high risk for heart surgery may be candidates for less invasive, catheter-based (percutaneous) options, such as MitraClip, Transcatheter Mitral Valve Replacement (TMVR) and Balloon Valvuloplasty.
What is mitral valve disease?
Mitral valve disease means the mitral valve, which is on the left side of your heart, between the top and bottom chambers, isn’t working the way it should. Mitral regurgitation (MR) is when blood leaks backwards through the mitral valve. Mitral stenosis means the valve opening is too narrow, and blood can’t flow as it should from the top left chamber of the heart (atrium) to the bottom left chamber (ventricle; the heart’s main pumping chamber).
Mitral regurgitation
There are two common types of MR — degenerative and functional.
Degenerative MR – Commonly called mitral valve prolapse or myxomatous mitral valve disease. The leaflet(s) (the flaps inside the valve that open and close to let blood flow through) and chordae (tough, fibrous strings attached to the leaflets) become stretchy. The leaflets become floppy and they do not close tightly. When this happens, surgery is the best treatment option. But, surgery is too risky for some patients. A newer treatment option, called the MitraClip, is approved by the Food and Drug Administration (FDA) to treat patients who are high-risk for surgery.
Functional MR – The mitral valve leaks due to a problem with another part of your heart, such as your left ventricle (may be too big or not working as it should), the ring attached to the leaflets (annulus) of the valve (may be too wide) or papillary muscles that support the leaflets (may be damaged). This damage can be caused by changes to the left ventricle after a heart attack or from diseased heart muscle (cardiomyopathy). If you have functional MR, your valve leaflets may be normal. Many patients with functional MR develop heart failure.
While surgery is the best treatment for patients with degenerative MR, it is not always the best treatment for patients with functional MR. MitraClip is also approved as a treatment for patients with functional MR.
What percutaneous treatment options are available for patients with MR?
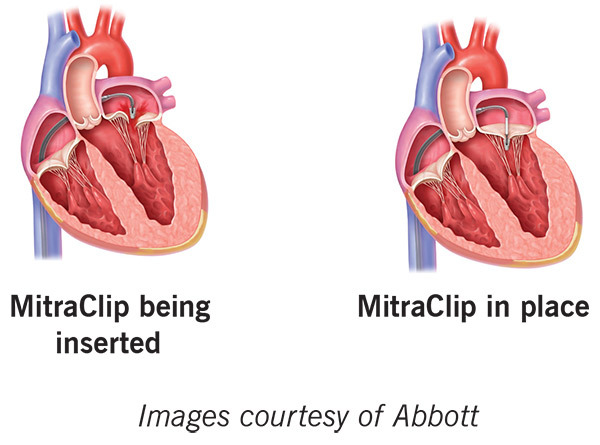
MitraClip
This procedure is also called edge-to-edge leaflet repair. The device lets the mitral valve close tightly, as it should.
MitraClip is a good option for patients who have:
- Degenerative or functional MR.
- A high risk of problems with traditional heart surgery.
- A valve structure that works well with the MitraClip.
- Heart failure and moderate-to-severe MR caused by problems with the left ventricle.
- Other tests, as needed.
Who can have percutaneous mitral valve treatments?
Nonsurgical treatment is not the best option for all patients. Each patient must have a detailed evaluation by a team of experts to determine what is best for them.
A team of doctors from different specialties will review your condition, current plan of care, past treatments and procedures, and overall health and quality of life.
The evaluation includes several tests, such as:
- Echocardiogram (echo): An ultrasound of your heart. A small amount of gel is placed on your chest, and a wand (transducer) is moved over your chest. Pictures of your heart are formed from the echoes sent by the transducer, and are displayed on a video screen.
- Transesophageal echocardiogram (TEE): An echo that takes pictures of your heart from inside your body. A long, thin tube (endoscope) is placed inside your "food pipe" (esophagus). A transducer on the end of the tube uses echoes to create pictures of your heart, and they are displayed on a video screen. This type of echo lets the doctor see your heart without your ribs and lungs blocking the view.
What can I expect if I am scheduled to get a MitraClip?
You will come to the hospital 1 to 2 days before your procedure. You will meet your surgeon, cardiologist, nurse practitioners and anesthesiologist. You will get detailed information and be able to ask any questions you have.
General information about the MitraClip procedure
- The procedure is done under general anesthesia.
- You will have a breathing tube (endotracheal tube) during surgery. The tube is removed when you can safely breathe on your own.
- The procedure takes 2 to 4 hours, plus prep and recovery time.
- The MitraClip is put in place with a long, thin tube called a catheter. The catheter is inserted through a small incision in your groin and guided through your femoral artery to your heart.
- The catheter is removed after the MitraClip is in place.
- You will stay in the hospital for 4 days after the procedure.
- You should be able to go back to your normal routine in about 2 weeks after the procedure.
- You will have 3 follow-up visits after the procedure: 30 days after the procedure, 6 months after the procedure and 1 year after the procedure.
Transcatheter Mitral Valve Replacement (TMVR)
Cleveland Clinic is using several types of transcatheter mitral valve replacement (TMVR) devices in carefully selected patients as part of clinical studies. This treatment is a possible option for patients with MR who cannot have a MitraClip procedure because of their valve anatomy or for those who have functional mitral regurgitation and are too high risk for conventional valve surgery.
What can I expect if I am scheduled to have TMVR?
You will come to the hospital 1 to 2 days before your procedure. You will meet your surgeon, cardiologist, nurse practitioners and anesthesiologist. You will get detailed information and be able to ask any questions you have.
General information about the TMVR procedure
- The procedure is done under general anesthesia.
- You will have a breathing tube (endotracheal tube) during surgery. The tube is removed when you can safely breathe on your own.
- The valve is put in place using a long, thin tube called a catheter. The catheter is inserted through a small incision between your ribs or your groin.
- The catheter, which has a sheath that holds the valve, is guided through an artery to your heart.
- The catheter is removed after the valve is put in place. The sheath is removed once your team checks to make sure the valve is working as it should.
Mitral Stenosis
When you have mitral stenosis, the tissues that form the valve leaflets become stiff and do not open all the way. The narrow valve opening causes less blood flow through it. The valve can become so narrow (stenotic) that it keeps the heart from working as it should, and the rest of the body may not get enough blood. If this happens, the valve may need to be repaired or replaced.
What percutaneous treatment options are available for patients with mitral stenosis?
Balloon Mitral Valvuloplasty
Balloon mitral valvuloplasty uses a tiny balloon attached to a catheter that is expanded to open the mitral valve and let blood flow through more freely. A small incision is made in your groin, and the catheter is guided to your heart through the femoral vein. A small incision is made in the wall between the heart’s upper chambers (atria) so the catheter can go into the valve. The balloon is inflated and deflated, then removed. If you are interested in this procedure, your doctor will talk to you about whether it is a good option for you.
Transcatheter Valve-in-Valve Replacement
Valve degeneration can happen after a valve replacement procedure with a bioprosthetic valve. Transcatheter mitral valve replacement is sometimes used to treat patients with this problem. This is called valve-in-valve (ViV) placement. Your doctor may talk to you about this treatment option if you have valve degeneration and:
- You have a bioprosthetic valve.
- Your valve opening is right for the procedure.
- You have a high risk of problems with traditional heart surgery.
- You do not have other valve problems that are best treated with cardiac surgery.
