You have been referred to a vascular surgeon because you have kidney disease and will need dialysis in the future. This dialysis will use a dialysis access, which requires a minor surgical procedure.
What is dialysis?
Dialysis is sometimes referred to as hemodialysis. It is used to treat patients with kidney failure. The process uses a machine that acts as a kidney to clean your blood and maintain the right amounts of fluids and chemicals in your body.
The process takes about 4 hours and is usually done 3 times each week.
What is dialysis access?
Dialysis access is an entry way to your bloodstream. The access is placed under the skin, usually in your nondominant arm. The access allows blood to be removed and cleaned, then returned to your body quickly, efficiently and safely. You may also hear the access called a shunt, graft or fistula.
Having an access in place before you need to start dialysis may eliminate the need for you to have a temporary catheter placed in your chest. If you have a temporary catheter in your chest, it can be removed after the access is in place. Early removal of the catheter lowers the risk of infection in your blood and heart. It also reduces the risk of damage and scar tissue in your veins.
A dialysis access does not affect how your kidneys work. Getting a dialysis access does not mean you will start dialysis right away.
Types of Access
There are three types of access —arteriovenous fistula (AVF), arteriovenous graft (AVG) and a temporary catheter.
Permanent options
Arteriovenous Fistula (AVF)
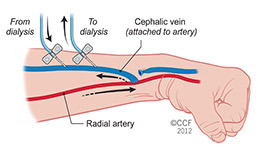
An AVF is created by joining an artery directly to a vein. The access is often placed in the arm (forearm or upper arm). Once the artery and vein are connected, more blood flows into your vein, which makes it bigger and stronger with time. It can take 3 to 6 months for the AVF to develop and be used during dialysis.
Your risk of infection is more than five times lower with an AVF than with an arteriovenous graft (AVG) and temporary catheter. There is also a lower risk of clotting.
Most people do not need to stay in the hospital overnight after having an AVF procedure.
Arteriovenous Graft (AVG)
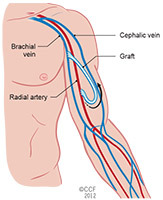
An AVF is the preferred type of dialysis access. But, your veins may be too small to have an AVF. If your veins are too small to form a good fistula, you may need an AVG. Like an AVF, an AVG involves joining an artery and vein. But, this is done using a man-made (synthetic) tube (graft). It is placed under the skin in your arm. The graft acts as a vein and, like an AVF, is used to put the dialysis needles in place. It takes 2 to 3 weeks before the access can be used for dialysis.
The risk of infection is higher with AVGs than with AVFs. This is because of the synthetic material used to make the graft.
Most people do not need to stay in the hospital overnight after having an AVG procedure.
Venous catheter
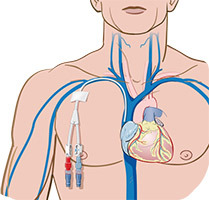
A temporary option for dialysis access is a venous catheter, also called a permacatheter or perm-cath. This is an option when you need to start dialysis right away. It is removed as quickly as possible and replaced with permanent access (AVF or AVG).
A catheter access involves placing a catheter (flexible, hollow tube) into a vein in your neck. The other end of the catheter is placed in your chest.
Catheters increase the risk of infection of your blood and heart. They can also cause damage to the vein, making it impossible to have a permanent access in that area.
Most people do not need to stay in the hospital overnight after having a venous catheter procedure.
What should I expect before the procedure?
Your surgeon may want you to have a venogram, ultrasound and/or circulation test to help determine which type of access is best for you.
Once it’s determined that you need an access, it’s important to have any testing you need and the surgery as soon as possible. This can help you avoid the need for a temporary catheter.
Before your surgery, you will meet with a vascular nurse for a pre-operative (pre-op) appointment. You will also visit the preoperative anesthesia consultation and evaluation (PACE) clinic.
What happens after the procedure?
Most patients are able to go home the same day they have their access surgery.
If you have an AVF or AVG
If you have an AVF or AVG, it is important that you follow the instructions you received when you left the hospital (discharge instructions). The following are also important to your recovery:
- Elevation: You may have swelling that will go away as you heal. Keeping your arm on a pillow to elevate it helps reduce the swelling and can help ease pain. Elevate your arm as often as possible until the swelling is gone.
- Pain control: Discomfort and pain after surgery should be mild and last only a few days. Your surgeon may prescribe pain medication or recommend that you take an over-the-counter pain reliever.
- Dressing and wound care: Keep the dressing in place for 24 hours after your procedure. After that, you can remove the dressing to look at your incision to check for signs of infection, then replace it with a new dressing.
- Activity: Do not lift anything that weighs more than 10 pounds or take part in any activity that could add stress to your access area for 1 to 2 weeks after surgery.
- Call your doctor if you have a fever higher than 101 degrees Fahrenheit, bleeding, pain that gets worse, swelling, or if you your hand feels cool or numb.
- If you have stitches, they will be removed in 10 to 14 days. At that time, you may get instructions for an exercise program to help develop your AV access. If you do not have external stitches, you will have a follow-up appointment 3 to 4 weeks after your procedure.
The To-Do List for Access Care
Taking care of your access
It is important to follow these instructions to help your access heal properly and prevent infection. Please call your doctor if you have any questions.
- DO keep the incision clean and dry until it is well-healed.
- DO remove the dressing 48 hours after your procedure and gently wash the incision with soap and water.
- DO feel the "thrill" with your fingertips at least once a day. We will show you how you should check your access site. The thrill can be felt over the fistula, using a light touch. The thrill feels like a cat purring or a motor running. It is a sign that your AVF is working.
- DO start doing AVF exercises 2 weeks after your procedure.

- DO call your surgeon or dialysis unit if:
- You do not feel the thrill.
- You have redness, tenderness or drainage at your access site.
- You have a fever or chills.
- Your hand is cold or numb.
- DO make an appointment to see your nephrologist after your access is in place.
The Do Not List for Access Care
- DO NOT sleep on the arm that has the access.
- DO NOT have blood drawn from the arm that has the access.
- DO NOT allow IVs to be placed in the arm that has the access.
- DO NOT check your blood pressure on the arm with the access.
- DO NOT carry heavy loads (including purses, babies, books,) on the arm with the access.
- DO NOT wear tight sleeves, watches or bracelets on the arm with the access.
How do I know if there are problems with my fistula or graft?
If you do not feel a thrill or pulse in your access, IMMEDIATELY tell a member of your dialysis team, nephrologist or vascular surgeon.
This is an emergency and means your access has closed. But, the problem can be corrected if it is treated right away.
The following may be signs of a problem with your fistula or graft. If you have any of these symptoms, tell a member of your dialysis team:
- The thrill that you feel changes to a pulse (like a heartbeat).
- There are more problems with infiltration than normal during dialysis.
- It takes longer for the bleeding to stop after the needles are removed during dialysis.
- There is a decrease in the "flow" or "clearance" with dialysis. This can be identified by the team at the dialysis center.
If your dialysis team confirms that there is a problem with your access, you will need to see your surgeon. You may need a procedure to correct the problem.
