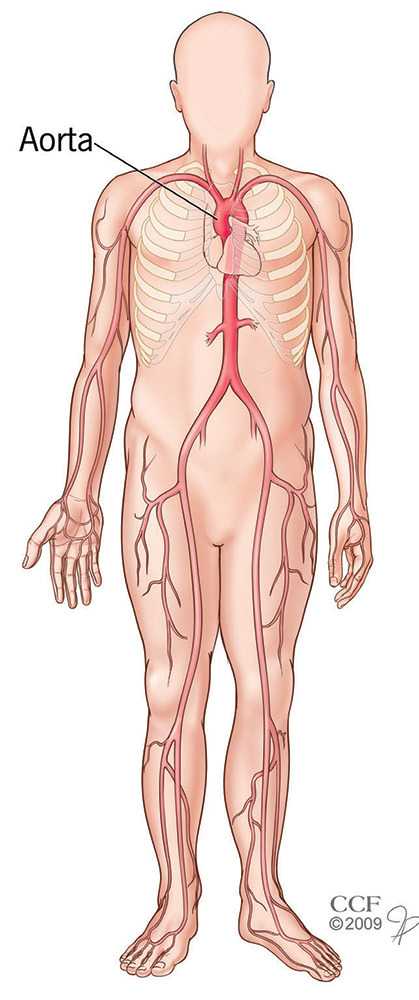
What is coarctation of the aorta?
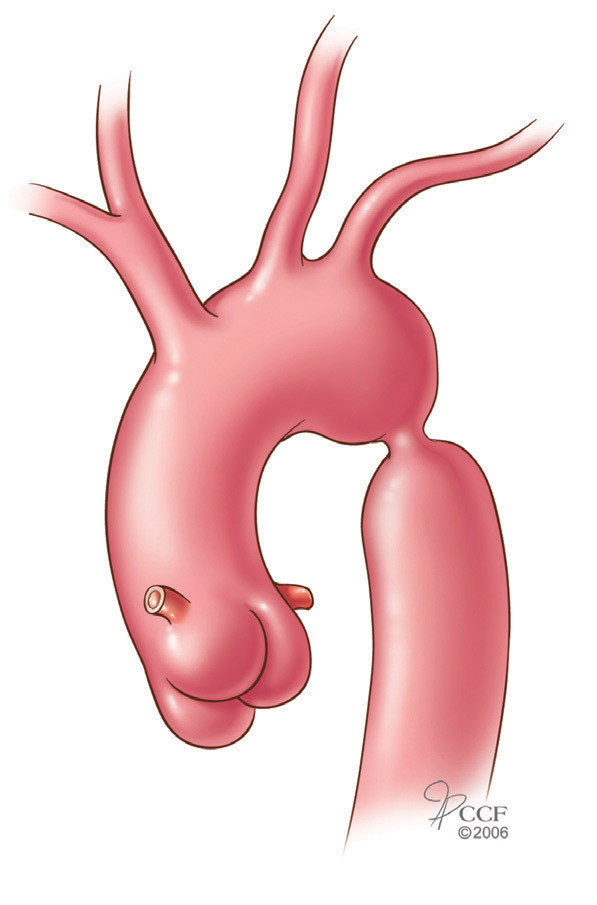
Coarctation of the aorta is a common congenital (present at birth) heart defect where the aorta is pinched in or narrowed, which restricts blood flow. The defect can affect a single spot or a larger section of the aorta.
Who is affected by coarctation of the aorta?
Coarctation of the aorta affects about 1 in 10,000 people and accounts for 5 to 10 percent of all congenital heart defects.
What are the long-term effects of coarctation of the aorta?
Coarctation of the aorta causes high blood pressure. Without treatment, the condition can lead to stroke, coronary artery disease at a young age, brain aneurysm, ruptured aorta, kidney failure and liver failure.
More than half of people with coarctation of the aorta also have a congenital heart valve defect (bicuspid aortic valve). The valve condition usually gets worse with time, and surgery may be needed to repair or replace the valve. People who have valve disease are also at risk for an aortic aneurysm —the walls of the aorta get weak, which causes it to bulge out and possibly rupture.
What are the symptoms of coarctation of the aorta?
Symptoms depend on how narrow the aorta is. Severe cases are often diagnosed at birth or within the first months of life. In mild cases, symptoms might not start until adulthood. Symptoms in an adult may include not being able to exercise, headache, shortness of breath, chest pain, nose bleeds, cold feet or leg pain after exercise.
How is coarctation of the aorta diagnosed?
Aortic coarctation usually happens between the area where the blood vessels branch off the aorta to the upper body and the area where the blood vessels branch to the lower body. Because of this, aortic coarctation causes high blood pressure in the arms and upper body and low blood pressure in the lower body and legs. This blood pressure difference is one of the most classic signs of the condition. Others include differences between the pulse at the groin and the neck and a distinctive harsh heart murmur that can be heard when a stethoscope is on the back.
If you have coarctation of the aorta, your cardiologist may order tests to find out how severe it is.
Tests include:
- Electrocardiogram (ECG).
- Chest X-ray.
- Echocardiography.
- Chest computed tomography (CT or CAT) scan.
- Magnetic resonance imaging (MRI) of the chest.
- Cardiac catheterization.
What treatments are available?
In the past, surgery was the only treatment available for patients with aortic coarctation. Surgery is still considered the gold standard, but treatment options for children and adults with this condition now also include balloon angioplasty and stenting. The choice of treatment is based on your overall health, the size and severity of the coarctation and its exact location.
If you have coarctation of the aorta, you should be under the care of an experienced congenital heart specialist at a major medical center. A cardiac surgeon experienced in the procedures used to treat patients with this condition can best determine the timing and type of treatment that is best for you.
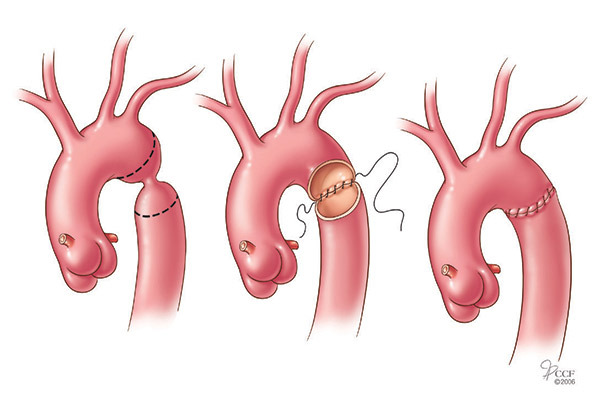
Surgery
When the coarctation is fairly small, the surgeon can remove the narrowed section of aorta and rejoin the two ends. This is called an end-to-end anastamosis and is often the best surgical treatment option.
Other types of surgery include various types of bypass surgeries in which a graft is stitched onto the aorta to move blood around the area of the defect. A bypass can be done at the same time as valve surgery, if needed.
Angioplasty
Angioplasty is another option for treating patients with coarctation of the aorta. The procedure is similar to angioplasty for patients with coronary artery disease. A long, thin tube called a catheter is placed into a blood vessel through a small incision in the groin. The catheter is guided into the aorta. A tiny balloon on the end of the catheter is inflated once the catheter reaches the coarctation. This opens up the narrow area of the aorta. Once the area is widened, the balloon catheter is removed.
A small metal mesh tube called a stent may be placed at the site of the coarctation to keep the aorta open. Stenting can lower your risk of an aneurysm and ruptured aorta. Your doctor will talk to you about the best treatment for you.
Recurring coarctation
There is a small risk after treatment that you can have aortic coarctation again. The risk for adults is between 5 and 10 percent after surgery. If you have angioplasty or stenting, the risk is between 11 and 15 percent for adults. Your doctor will talk to you about the benefits of the procedure as well as the risk of complications. If coarctation does happen again after any treatment, angioplasty with stenting is the preferred treatment.
Follow-up care
Ongoing care from a congenital heart disease specialist is very important after treatment for aortic coarctation. This includes regular visits to check your blood pressure and a yearly exam. You should also have Doppler ultrasound and MRI tests every two to five years.
If your blood pressure is normal after treatment, you probably won’t have any activity restrictions. But, if your blood pressure stays high, you will most likely need to avoid some strenuous activities and sports.
Coarctation of the aorta and endocarditis
After heart surgery or angioplasty to repair a defect, you will need to take antibiotics before certain medical procedures for at least 6 months after the procedure. This is to reduce your risk of getting infective endocarditis. Your doctor can give you detailed information about prevention and antibiotic use.
References
- Ebeid MR, Prieto LR, Latson LA. Use of balloon-expandable stents for coarctation of the aorta: Initial Results and Imtermediate-Term Follow-Up. J Am Coll Cardiol. 1997;30:1847-52.
- Ebeid MR, Sarris GE, Drummond-Webb JJ, Prieto L, Ratliff NB, Latson LA. Immediate post-operative balloon dilatation of neonatal long segment stenosis of the descending thoracic aorta. J Invas Cardiol. 2001;13:44-46.
- Godart F. Management of aortic coarctation at the adult age- Article in French] Archives des Maladies du Coeur et des Vaisseaux. 2007 May; 100(5):478-83.
- Hamdan MA, Maheshwari S, Fahey JT, Hellenbrand WE. Endovascular stents for coarctation of the aorta: initial results and intermediate-term follow-up. Journal of the American College of Cardiology. 2001 Nov 1; 38(5):151823.
- Hassan W, Awad M, Fawzy ME, Omrani AA, Malik S, Akhras N, Shoukri M. Long-term effects of balloon angioplasty on left ventricular hypertrophy in adolescent and adult patients with native coarctation of the aorta. Up to 18 years follow-up results. Catheterization and Cardiovascular Interventions. 2007 Nov 15; 70(6):881-886.
- Karl TR. Surgery is the best treatment for primary coarctation in the majority of cases. Surgery is the best treatment for primary coarctation in the majority of cases. Journal of Cardiovascular Medicine (Hagerstown). 2007 Jan; 8(1):50-6.
- Koerselman J, de Vries H, Jaarsma W, Muyldermans L, Ernst JM, Plokker HW. Balloon angioplasty of coarctation of the aorta: a safe alternative for surgery in adults: immediate and mid-term results. Catheterization and Cardiovascular Interventions. 2000 May; 50(1):28-33.
- Krasuski RA, Fouad-Tarazi, F. “Coarctation of the aorta.” 923-30. Comprehensive Hypertension. Lip GYH and Hall JE, eds. Philadelphia, PA: Mosby, Inc., 2007.
For more information
- Adult Congenital Heart Association, www.achaheart.org, 888.921.ACHA.
- American Heart Association, www.americanheart.org, 800.242.8721.
- Congenital Heart Information Network, 609.822.1572.
- International Society for Adult Congenital Cardiac Disease, www.isachd.org, 919.861.5578.
Sydell and Arnold Miller Family Heart & Vascular Institute
The Miller Family Heart & Vascular Institute specialists are among the most experienced in the world in treating adults with congenital heart defects. Our team approach ensures that patients receive the best care before, during and after their procedure.
