Tourette syndrome is a disorder that causes uncontrollable movements and vocal sounds called tics. It often shows up in early childhood and improves in adulthood. Tics can be mild or severe. Medication and therapy can help reduce tics.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Tourette syndrome (TS) is a neurological disorder that affects your brain and nerves. It causes you to make sudden movements or sounds called tics. Tics are involuntary, so you can’t control or prevent them. Motor tics involve body movements, like eye blinking or shoulder shrugging. Vocal tics involve your voice, like sniffing or throat clearing. Motor tics tend to develop before vocal tics.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Tourette syndrome, or Tourette’s, usually starts in early childhood. Most of the time, tics become milder and occur less frequently in late adolescence and adulthood. Tourette syndrome is the most severe type of tic disorder.
Tourette syndrome affects 1 out of every 160 children, which means that approximately 300,000 children in the U.S. have the condition.
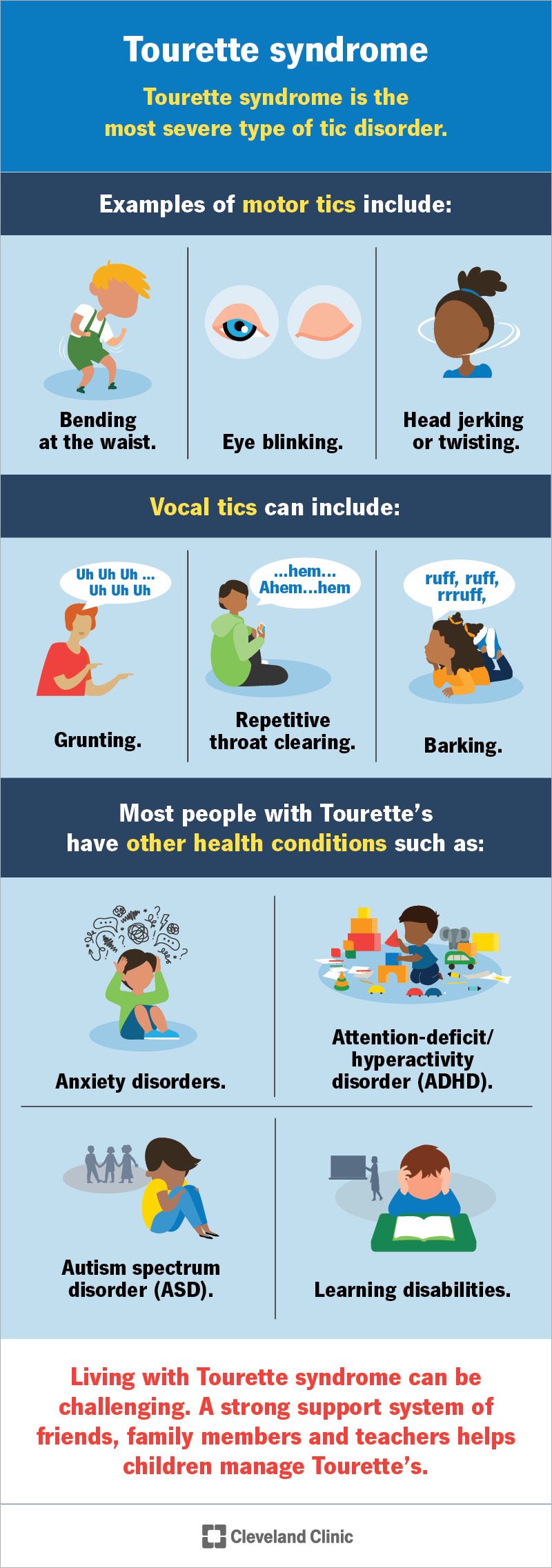
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/tourette-syndrome)
The most common Tourette syndrome symptoms are motor and/or vocal tics. Tics usually start between the ages of 5 and 7 and peak around age 12.
Tics are either simple or complex:
Researchers don’t know the exact cause of Tourette syndrome. But the condition tends to run in families, so they believe genes may play a role. Issues with how your brain breaks down (metabolizes) neurotransmitters may also contribute to Tourette syndrome. Neurotransmitters, like dopamine, are chemicals in your brain that regulate behavior and movement.
Risk factors for Tourette syndrome may include:
Advertisement
Most people with Tourette’s have other health conditions. These are usually mental or behavioral health disorders, including:
To diagnose Tourette syndrome, a provider checks when the tics started. They should begin before age 18. Your child must have both motor and vocal tics for over a year.
There isn’t a blood test or imaging exam that can detect Tourette syndrome. Instead, your child’s provider will carefully review their medical history and symptoms.
Their provider may also do tests to rule out other conditions that could be causing tics.
Mild tics that don’t affect your child’s everyday activities might not need treatment. But severe tics can make it hard to function at work, school or in social situations. Some tics can even lead to self-injury. In these cases, Tourette syndrome treatment, including medication or behavioral therapy, may help.
For mild tics, your child’s healthcare provider may recommend medications that typically treat high blood pressure. These medications include clonidine and guanfacine.
For more severe tics, your child’s provider may recommend neuroleptics (antipsychotic medication). Neuroleptics are drugs that limit the activity of dopamine in your brain. Dopamine is a chemical that can increase tics.
Other medications can help manage conditions that occur with Tourette’s, like ADHD or OCD.
The tics associated with Tourette’s are involuntary, so they aren’t something you or your child can control. But new therapies help people manage tics and reduce their negative effects.
Comprehensive behavioral intervention for tics (CBIT) helps people:
Advertisement
Contact a healthcare provider right away if someone with Tourette syndrome:
You can call or text the Suicide and Crisis Lifeline at 988.
There’s no cure for Tourette syndrome. The condition usually improves by early adulthood. Tics may still occur, but most adults don’t need to continue medication or therapy.
People with Tourette syndrome have a typical life expectancy. Tourette syndrome isn’t a progressive condition — it doesn’t get worse over time. In many cases, the condition is mild and the tics go away on their own.
Tics among children aren’t uncommon, and they’re usually harmless. But if you notice your child’s tics becoming more severe or frequent, it’s possible they may have Tourette syndrome (TS). If you can, take a video of your child performing their tic so you can show it to their healthcare provider. Your child’s provider can determine if Tourette’s is affecting your child and recommend appropriate treatment.
It’s important to remember that your child can’t control their tics. Their tics make them unique. Make your friends, loved ones and child’s teachers aware of your child’s tics so they understand the condition. And work with your child’s provider to get them the best possible treatment to manage their tics.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Parkinson’s disease, essential tremor and dystonia are common movement disorders. And Cleveland Clinic has the expert care and support you need to manage them.
