A hemispherectomy is a rare surgery that either removes or disconnects half of the brain from the other half. It treats mostly children and some adults who have seizures that don’t respond to medicine. Following the surgery, you’ll be in the hospital for five to seven days and then will go through a period of rehabilitation.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A hemispherectomy is an operation that partially or completely removes or disconnects half of your child’s brain from the rest of their brain. It’s a rare procedure a surgeon performs in a hospital. Children (and occasionally adults) typically have this procedure for epilepsy that doesn’t respond to medications. In people with this issue, the whole hemisphere is abnormal and responsible for causing seizures.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The “hemi” part of “hemispherectomy” means “half” and refers to the cerebral (brain) hemisphere — half of your brain. You may also hear the surgery called a radical hemispherectomy.
There are two types of hemispherectomies: anatomic and functional (disconnective).
The two types of surgeries have equal success. However, when a functional hemispherectomy doesn’t stop seizures, following up with an anatomic hemispherectomy can lead to freedom from seizure in one-third of children who have the surgery.
Your child might need a hemispherectomy if they have these symptoms:
Advertisement
These symptoms can be signs of the following conditions and diseases:
Your child might have started having seizures and weakness early in life. Their provider may suspect drug-resistant epilepsy and will refer you to a center that specializes in children with seizures.
Your child’s provider will give you information on what to do before the surgery. This generally involves no food or water after a certain time the day before. They’ll also give you directions on what medications they should take or stop taking.
Your provider or a child life specialist may help you find ways to support your child at this time. You might need words to explain simply what’s going on if your child is old enough to understand.
A provider will wash your child’s hair so that it’s clean. A member of the healthcare team will cut or shave your child’s hair over part of their head.
Your child will have general anesthesia so they won’t feel pain during the procedure. During the surgery, their surgeon will:
Typically, the procedure takes about five hours, but it can take longer. You may want to have someone waiting with you during the surgery. Usually, you’ll receive updates periodically.
Advertisement
A healthcare team will monitor your child in the recovery room and later in the intensive care unit (ICU).
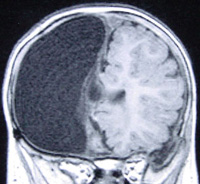
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/hemispherectomy-coronalmriA_1_)
Coronal MRI following right anatomic hemispherectomy.
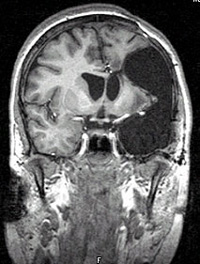
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/hemispherectomy-postopmri)
In left functional hemispherectomy, certain areas of the brain responsible for muscle movement are removed.
Typically, a hemispherectomy is a successful treatment. Different studies indicate that between two-thirds of children (over 66%) to more than 80% of children who undergo hemispherectomy are completely seizure-free. Most of the rest of the children who have hemispherectomy have fewer seizures after the operation.
If your child has persistent seizures after an initial procedure, your provider will do a careful evaluation to see if they could benefit from a repeat surgery.
The best results seem to happen for children who have few or no seizures after the surgery.
Most children have excellent long-term results following a hemispherectomy. But occasionally, some complications or negative effects may occur.
Early complications, which can happen during or immediately after the operation, can include:
One complication that can occur early or later in life is hydrocephalus, or fluid buildup in the brain. This happens in less than 5% of people who have a functional (disconnective) hemispherectomy.
Advertisement
The risk of hydrocephalus is a little bit higher if you have an anatomic hemispherectomy. If hydrocephalus happens, your child will need a shunt to help remove the fluid.
Another complication is excessive blood loss. If this happens, your child might need a blood transfusion.
After this epilepsy surgery, your child will spend at least two to three days in the pediatric intensive care unit for close monitoring. Your child will continue to receive antiepileptic medications.
Your child may have a brain CT or MRI on the first morning after the operation to assess their brain. Caregivers will remove the surgical drains and transfer your child to a regular pediatric nursing floor after the intensive care stay.
Their healthcare team will contact specialists to help your child regain the skills they need for everyday activities and communications. These are specialists in:
An average hospital stay slightly varies among individuals and usually ranges from five to seven days. Their surgical team makes length-of-stay decisions based on your child’s condition and recovery.
Upon discharge, children often need rehabilitation services to enhance their recovery from hemispherectomy. Your child may transfer to a rehab facility for intensive physical, occupational and speech therapy.
Advertisement
After that, they usually have home or outpatient services. Hospitals, free-standing facilities and schools can provide outpatient therapy. Check with your individual school system to see if this is a service they provide.
You may wonder what your child’s life will be like after a hemispherectomy. They may need this support after surgery, but the side of their brain that works well has already taken over for the affected side. Outcomes are good for walking, reading and behavioral issues, but some vision loss will happen.
Your surgeon will give you information on when you should call or go to the emergency room after a hemispherectomy. You should feel free to call any time you’re concerned about signs or symptoms.
Typically, call your provider or get emergency help if your child:
In general, people with epilepsy may have a shorter lifespan, but this isn’t always true. Stopping the seizures with the hemispherectomy is likely to improve quality of life and possibly length of life as well.
When someone with repeated seizures can’t get relief from medication, a provider may recommend a hemispherectomy. No provider would give this recommendation lightly. However, the success of the operation is high, and the benefits are considerable. Speak with the members of your child’s healthcare team to learn as much as you can. Ask for help whenever you need it. There are services and providers who’ll work with you before, during and after a hemispherectomy.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.