Carpal tunnel syndrome is an extremely common wrist issue. Irritation or damage inside the carpal tunnel in your wrist causes it when swelling presses on your median nerve. Carpal tunnel syndrome symptoms include wrist pain, tingling, numbness and weakness. A healthcare provider will suggest treatments like wearing a splint, physical therapy or surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
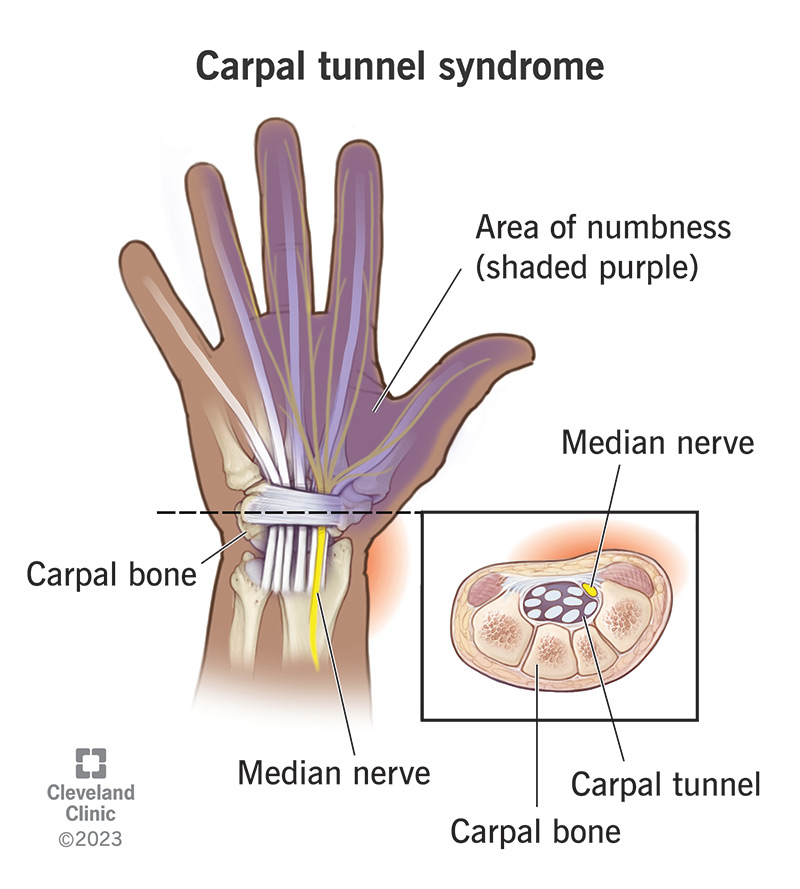
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/carpal-tunnel-syndrome)
Carpal tunnel syndrome is a health condition that causes symptoms like pain, numbness, tingling and weakness in your hand and wrist.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The carpal tunnel is a space in your wrist bones. It’s like a tunnel road through a mountainside, but instead of making room in the rock for cars, it’s a passageway in your bones that lets tendons, ligaments and nerves pass through it to reach your hand.
Carpal tunnel syndrome happens when something irritates or puts extra pressure on the median nerve that runs through your carpal tunnel. The median nerve helps you move your forearm and gives feeling to most of your fingers and hands. If it’s damaged or pressed against the walls of your carpal tunnel, it can send extra or incorrect feelings to your hand and wrist.
Visit a healthcare provider if you’re experiencing pain, numbness or tingling in your hands and wrists. Carpal tunnel syndrome usually responds well to treatment, but it can permanently damage your median nerve if it’s not treated soon enough.
Carpal tunnel syndrome is extremely common. Experts estimate that around 3 out of every 1,000 people in the U.S. experience carpal tunnel syndrome each year.
The most common carpal tunnel symptoms include:
Advertisement
Carpal tunnel syndrome usually develops slowly. You might only experience minor symptoms at first that may get worse over time.
People usually first notice symptoms at night — pain or tingling may wake you up. Over time, the symptoms may start affecting you during the day, especially if you do the same kind of motion a lot at work like typing, writing or using tools.
Carpal tunnel syndrome can make your wrists, hands and fingers feel uncomfortable. It may feel like pinpricks or like your fingers or hands “fell asleep.” You may also feel numbness that makes you want to shake your hands like you’re flinging water off them.
Carpal tunnel syndrome pain usually feels like it’s coming from inside your hand or wrist — not a skin-level pain like a cut. The pain may feel like a sharp, burning stab or a constant ache.
Some people with carpal tunnel syndrome feel like their hands and grip are weaker than normal. It might feel like you can’t get a solid hold on a mug or pen, even if you’re concentrating on it.
Your hands and fingers may feel clumsy or less able to perform precise motions, like buttoning a shirt or aiming a key into a lock.
Extra pressure on your median nerve causes carpal tunnel syndrome. The carpal tunnel has space for all the parts that pass through it, but if one part of your wrist is swollen or damaged, it can press on other tissue around it, including your median nerve.
Anything that causes swelling or irritation in your wrist can cause carpal tunnel syndrome:
Anyone can develop carpal tunnel syndrome, but some people are more likely to, including:
Having certain health conditions can increase your carpal tunnel syndrome risk, including:
If a healthcare provider doesn’t diagnose and treat carpal tunnel syndrome as soon as possible, the irritation in your wrist can cause permanent damage. Specifically, the extra pressure can damage your median nerve, which may make it hard or impossible to feel, move or use your hand.
Visit a healthcare provider as soon as you notice carpal tunnel symptoms or any changes in how you can feel or use your hand and wrist.
A healthcare provider will diagnose carpal tunnel syndrome with a physical exam and some tests. They’ll examine your wrist, hand and fingers and ask about your symptoms. Tell your provider when you first noticed symptoms and if any activities or time of day make them better or worse.
Advertisement
Your provider will use a combination of physical and imaging tests to diagnose carpal tunnel syndrome, including:
Providers treat carpal tunnel syndrome with nonsurgical (conservative) treatments first. You may need carpal tunnel surgery if conservative treatments don’t relieve your symptoms.
The most common carpal tunnel treatments include modifying your daily routine, supporting and strengthening your wrist and taking medication:
Advertisement
If conservative treatments don’t work, your provider will suggest carpal tunnel surgery. Your surgeon will perform a carpal tunnel release to create more space inside your wrist. They’ll make an incision (cut) in the ligament that connects your wrist to your palm (your transverse carpal ligament). This reduces tension on your carpal tunnel and gives your tendons and nerves more space.
Carpal tunnel release surgery is usually an outpatient procedure, which means you can go home the same day. Your surgeon will tell you what the expect and will give you recovery instructions.
You should start feeling better as soon as you start carpal tunnel treatment. It might take a few weeks (or longer) for nonsurgical treatments to reduce the pressure on your median nerve, but your symptoms should start improving gradually.
Carpal tunnel surgery should improve your symptoms as soon as your wrist heals. It usually takes a month or two to recover.
You should expect to tweak some of your daily activities and try a few nonsurgical treatments to support your wrists and reduce inflammation inside your carpal tunnel. Your healthcare provider will suggest treatments that relieve carpal tunnel syndrome symptoms and prevent median nerve damage.
Advertisement
It might take a few tries to find treatments that work for you, but most people are able to find carpal tunnel relief. Your provider will suggest surgery if conservative treatments aren’t working or if you have severe carpal tunnel syndrome.
It can be hard to prevent carpal tunnel syndrome, especially if a health condition or activity you can’t avoid causes it. You might be able to reduce your risk by protecting your wrists. Protective steps include:
It’s possible for carpal tunnel syndrome to get better on its own — especially if you rest or avoid repetitive motions with your wrists for a while. But it’s much more likely that carpal tunnel syndrome won’t heal unless a healthcare provider diagnoses and treats it.
It’s not worth risking permanent damage to your median nerve. See a healthcare provider as soon as you notice any tingling, pain or numbness in your wrists, hands or fingers.
There’s no one answer that applies to everyone. Which treatments will work best for you depends on what’s causing irritation in your carpal tunnel, as well as the carpal tunnel syndrome’s severity.
Most people can manage carpal tunnel syndrome with conservative treatments. But surgery is sometimes the best option. There’s no one right or wrong answer when it comes to your health. A healthcare provider will help you understand which treatments are right for you and why.
Everyone experiences carpal tunnel syndrome differently. You might first notice symptoms at night, like wrist pain or tingling that are intense enough to wake you up. You may also notice that your wrists start showing signs of carpal tunnel the longer you use them, like at the end of a long day of working with tools.
Only a healthcare provider can confirm that you have carpal tunnel syndrome or another wrist issue. Even if you don’t have carpal tunnel syndrome, they’ll help you understand what’s causing the symptoms and how you can treat them.
Anything that affects your ability to feel and use your hands and fingers can be scary, annoying and frustrating — and carpal tunnel syndrome is no different. It happens when irritation causes extra pressure on the median nerve in your wrist.
It might seem easy to ignore occasional pain, tingling or numbness in your hand, especially if it comes and goes. But don’t shrug off these symptoms. Carpal tunnel syndrome can cause permanent nerve damage if it’s not treated soon enough. But it’s also very treatable. Your provider will help you find ways to relieve your symptoms and prevent damage inside your wrist.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
From sudden injuries to chronic conditions, Cleveland Clinic’s orthopaedic providers can guide you through testing, treatment and beyond.
