Uterine inversion is a rare but serious childbirth complication where your uterus turns partially or entirely inside out after delivery. Without treatment, an inverted uterus can lead to severe blood loss, shock and even death. Having a care team that’s prepared for emergencies can prevent these outcomes from happening.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
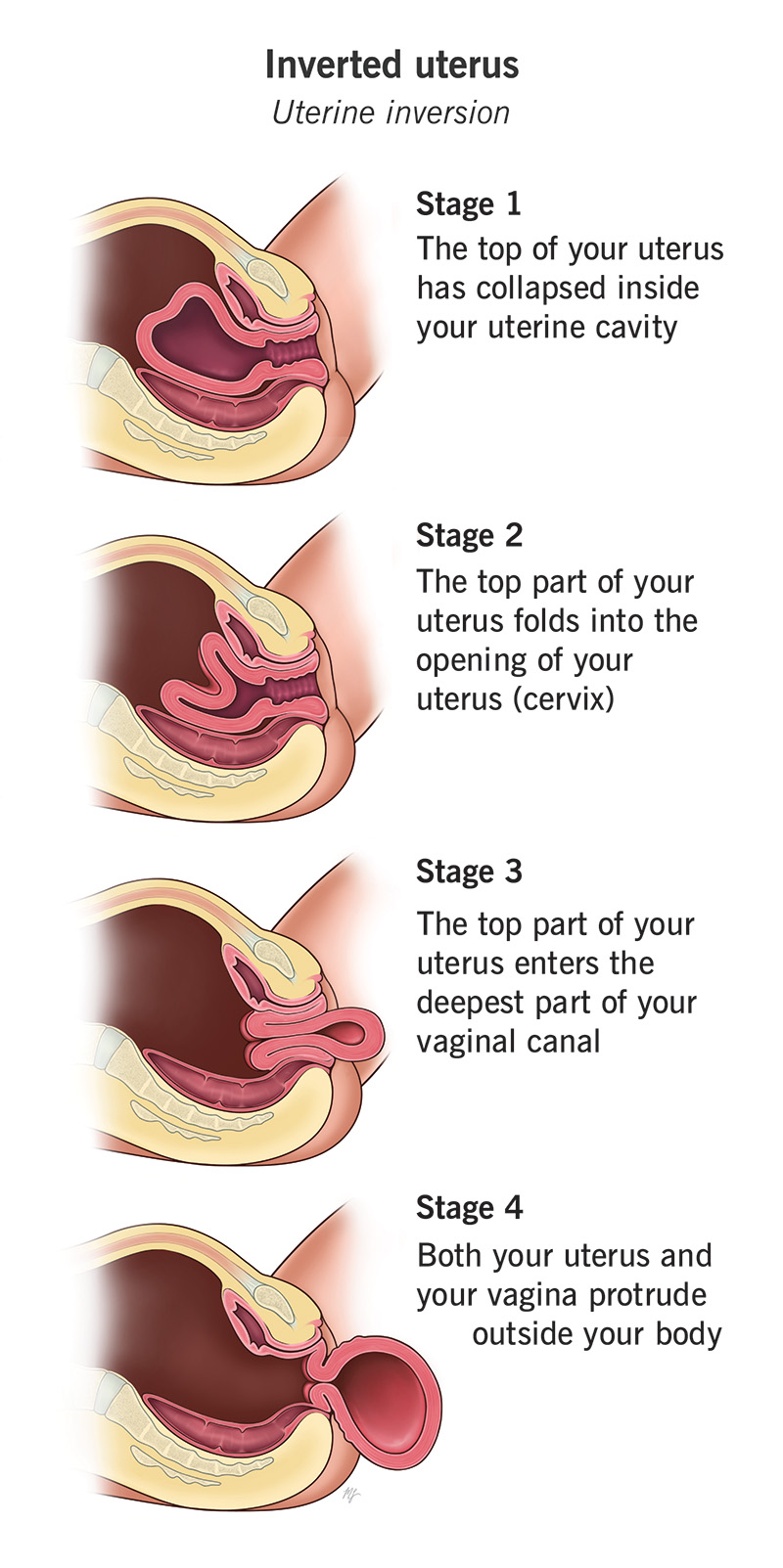
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/22326-uterine-inversion)
Uterine inversion is a rare and serious childbirth complication where your uterus turns inside out. Instead of maintaining its normal shape after delivery, your uterus collapses inward. It may even fall outside your vagina. It can cause severe blood loss, shock and possible death. A prepared care team that acts quickly can prevent these outcomes.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Most often, it occurs within the first 24 hours of delivery. In extremely rare cases, it happens for a reason other than childbirth.
Uterine inversion is a medical emergency. Symptoms can vary, depending on how extreme the inversion is. Some of those symptoms are:
You can also show signs of shock from losing too much blood. Symptoms could include:
Uterine inversion can sometimes happen after birth, when the placenta is being delivered. This process usually doesn’t cause any issues. But in rare cases, inversion can occur if you have certain risk factors that make it more likely.
Potential risk factors for uterine inversion are:
Your healthcare provider may be able to diagnose an inversion just by looking. A visible uterus and heavy bleeding are telltale signs of an inverted uterus. Your provider may feel your abdomen to see if your uterus has shifted out of place. They’ll also watch your vital signs to see if your blood pressure is dropping.
Advertisement
Diagnosis has to happen quickly so that lifesaving treatment can begin immediately.
The four types are:
Most uterine inversions fall into the 2nd- or 3rd-degree categories.
Successful treatment depends on your provider’s ability to act quickly to keep your vitals stable while the top of your uterus is placed into its original position. The care you receive depends on the degree of inversion. It may involve:
Uterine inversion can be life-threatening if your healthcare team can’t manage it. The survival rate is excellent, though, with a care team that’s prepared for emergencies. You can go on to lead a healthy life with no long-term complications.
Yes. You should tell your provider if you have a history of uterine inversion. This can help guide your care plan during a future pregnancy and delivery.
No. While both involve your uterus shifting or moving, an inversion means your uterus is collapsing or inside out. It’s a rare, life-threatening emergency that happens after childbirth. A prolapse is when your uterus slips down into your vagina. It can be severe, but it’s not life-threatening.
It’s unlikely that you’ll experience uterine inversion. If you do, having a care team that provides treatment right away can save your life. Talk to your provider about any concerns you may have about emergency complications, like uterine inversion. Ask about the protocols in place for lifesaving care if an emergency arises. This can give you peace of mind leading up to delivery.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic childbirth experts coach you through every step — from labor to delivery to what to expect when you and your newborn head home.
