Psoriatic arthritis is arthritis that’s linked to psoriasis, a chronic skin condition. The most common symptoms are joint pain and stiffness, skin rashes, and changes in your fingernails and toenails. There’s no cure for psoriatic arthritis, but treatments can manage the symptoms and reduce how often you experience flare-ups.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Video playlist content: This video playlist is available to watch online.
View video playlist online (https://cdnapisec.kaltura.com/p/2207941/sp/220794100/playManifest/entryId/1_qg0j86ei/flavorId/1_5f3sgelj/format/applehttp/protocol/https/a.mp4)
Learn more about psoriatic arthritis, its symptoms and possible treatment options.
Psoriatic arthritis (PsA) is a type of arthritis that affects people who have psoriasis or a biological family history of psoriasis.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
If you have PsA, you’ll experience symptoms of both arthritis and psoriasis. Arthritis causes pain and inflammation in and around your joints. Psoriasis causes inflammation in your skin. Psoriasis rashes are patches of discolored skin covered with scales. These thick, scaly areas are called plaques. It can also change how your fingernails and toenails look.
Visit a healthcare provider if you notice new symptoms on your skin or pain, swelling or stiffness in your joints.
A healthcare provider might classify PsA based on which joints it affects or which side of your body you experience symptoms. The five forms of psoriatic arthritis include:
Advertisement
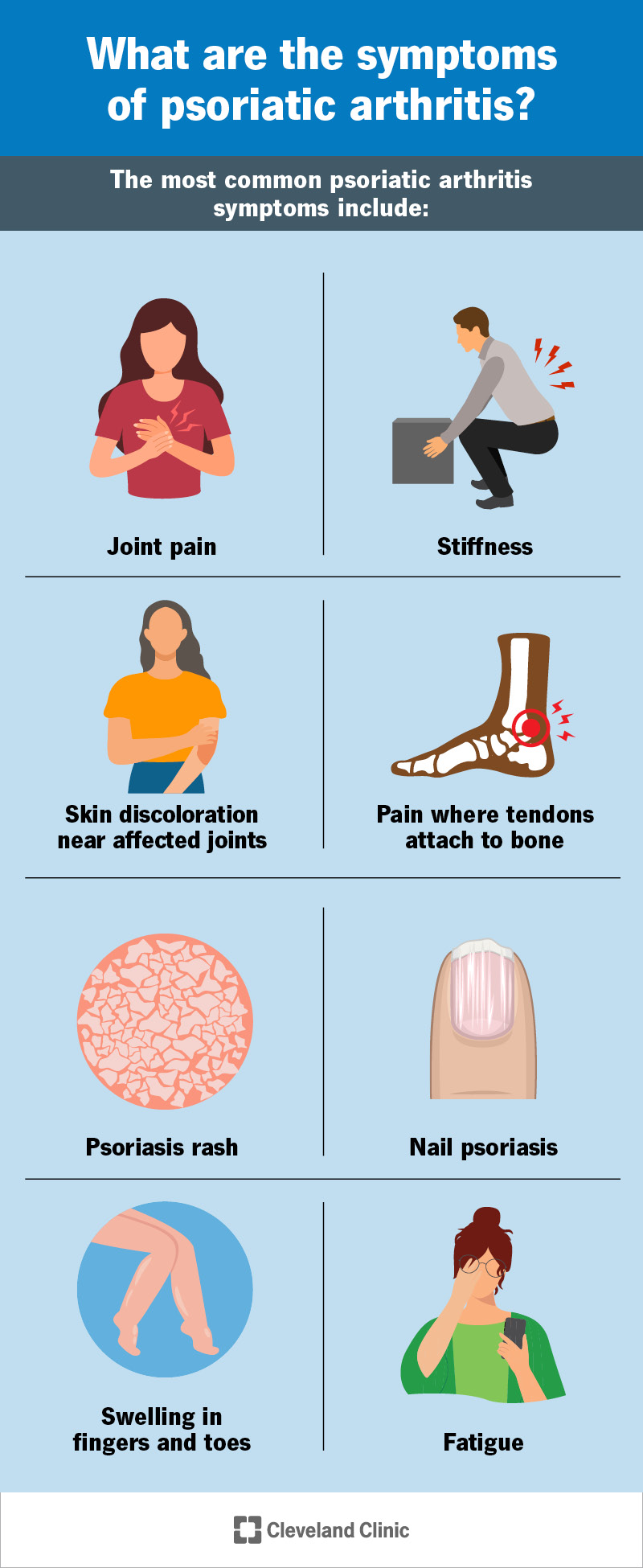
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/psoriatic-arthritis-infographic)
The most common psoriatic arthritis symptoms include:
PsA symptoms come and go in periods called flares or flare-ups. You might notice signs of a flare-up before one happens. You might feel mild symptoms that get worse before you enter a flare.
The severity of symptoms can vary between flares. More severe flares can make it hard to move and use your joints. They can also cause larger patches of psoriasis on your skin.
Psoriatic arthritis is an autoimmune disease. These happen when your immune system accidentally attacks tissue in your body instead of protecting it.
Experts aren’t sure what makes your immune system do this. Some studies have found that people with psoriatic arthritis have similar genetic changes. Experts can’t say for certain if these changes cause psoriatic arthritis. It’s possible they change after you develop it.
Around 4 in 10 people with psoriatic arthritis also have a biological family member who also has it. This means it might be an inherited genetic disorder. Tell your healthcare provider if you know that someone in your family has psoriasis or PsA.
You may have a higher risk of PsA if you have psoriasis. Around 1 in 3 people with psoriasis also get psoriatic arthritis.
People who get psoriatic arthritis usually develop psoriasis in their teens or early 20s, but don’t experience joint symptoms until later in life. Arthritis symptoms usually first show up between ages 30 and 50.
Having PsA can increase your risk of other health conditions, including:
Psoriatic arthritis symptoms can make it hard or painful to use your joints. This can make it tougher to do physical activities. Talk to a healthcare provider about low-impact exercises that put less pressure on your joints. Yoga, walking or aqua therapy are all good ways to stay active without stressing your joints.
A healthcare provider will diagnose psoriatic arthritis with a physical exam and some tests. Your provider will look at your skin and joints. Tell them which symptoms you’ve noticed, and if they come and go.
Advertisement
There’s no test that can diagnose psoriatic arthritis. But your provider might use tests to rule out other issues that can cause similar symptoms. For example, blood tests can show signs of infections.
Imaging tests can take pictures of your joints to show damage or inflammation. You might need:
Your healthcare provider will suggest treatments to manage the symptoms you experience. What’s best for you depends on a few factors, including:
You might need to visit a rheumatologist, a provider who specializes in treating autoimmune diseases. A skin specialist, like a dermatologist, can diagnose and suggest treatments for psoriasis symptoms.
The most common treatments for psoriatic arthritis include:
It’s very rare to need surgery if you have psoriatic arthritis. You might need a joint replacement if your joints are damaged or lose too much bone tissue. Your provider or surgeon will tell you which type of surgery you’ll need and what to expect.
Advertisement
Visit a healthcare provider if you notice new rashes or other symptoms on your skin, or if you’re experiencing joint pain. Talk to your provider if you notice changing symptoms. Tell them if psoriatic arthritis flares happen more often, or if they seem like they’re getting worse.
You should expect to manage PsA symptoms for the rest of your life. There’s no cure for psoriatic arthritis. But you may experience long periods of time between flares, especially once you find treatments that work well.
It can be frustrating when a flare happens suddenly. You’ll learn to recognize the warning signs of a flare and start managing the symptoms before they become more severe. Talk to your healthcare provider if you feel like your current treatments aren’t managing symptoms well enough.
Managing a chronic condition like psoriatic arthritis can be hard work. You might feel like you’re dealing with two conditions at the same time — the skin and nail symptoms of psoriasis and joint issues from arthritis. Your healthcare provider will help you find treatments that manage your symptoms during flares. They’ll also suggest ways you can keep your body healthy and strong to support your joints and skin.
You won’t feel your best every day. Try to give yourself some grace. Learning how to manage PsA is a skill that you’ll master over time. Listen to your body, and don’t hesitate to ask for adjustments in your treatment.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
From painful, swollen joints to irritated, scaly skin, psoriatic arthritis can complicate life. Cleveland Clinic is here to help you manage this condition.
