Locations:
An abdominoperineal resection (APR) is surgery that removes your sigmoid colon, rectum and anus. Surgeons do this in cases where a tumor is in your lower rectum. The surgery changes how you poop, so you’ll receive a colostomy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
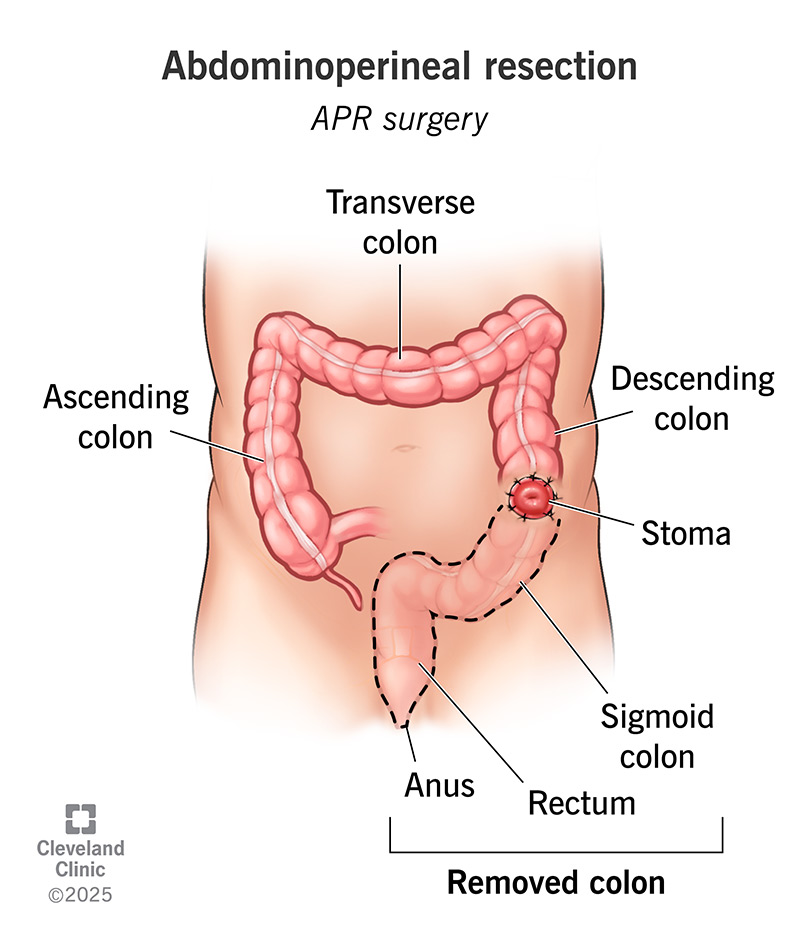
An abdominoperineal resection (APR) is a type of surgery that your surgeon may do to treat rectal cancer. In an APR, your surgeon may remove your anus (butthole), rectum and part of your colon. They’ll also do a permanent colostomy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
An APR is a major surgery. There’s a lot that goes into getting ready for it. Your care team will let you know if you need tests or other appointments before your surgery. Tests may include blood tests and imaging tests, like CT scans or MRI scans.
You may have other appointments to meet with your anesthesia team and other healthcare providers. They’ll help make sure you’re ready for surgery. You may meet with other surgeons who may participate in your surgery.
You’ll also meet your ostomy nurse. They’ll explain what an ostomy is and how to care for it. They’ll discuss places on your belly where an ostomy may go and pick the spot that’s best for it.
Your care team will explain what you need to do to get ready for surgery. For example, they’ll:
Having OSA increases your risk of anesthesia complications. If you use a CPAP device, they’ll ask you to bring it with you the day of your surgery.
Advertisement
They’ll tell you to start a clear liquid diet the day before your surgery and do bowel prep the morning of your surgery.
You’ll receive general anesthesia so you’re asleep during surgery. The surgery involves several steps. Your surgeon will:
Your surgery will take several hours.
An APR is major surgery with significant potential risks, including death. The risks of the operation can include:
You may need more surgery to manage complications. You may also have long-term complications, including an infection in your pelvis. You may develop a hernia around the ostomy or in the area where your anus and rectum were located. This is a perineal hernia.
You’ll remain in the hospital for several days after your surgery. You’ll have a catheter to drain pee from your bladder. Your care team will remove the catheter after a few days so you can pee on your own. You’ll also have a drainage tube in your belly that your care team will eventually remove. Your team will give you pain medications.
You’ll be able to drink fluids after your surgery. You’ll be able to eat soft foods the day after your surgery. You’ll also be able to get out of bed and walk.
You’ll have one-on-one teaching sessions with your ostomy nurses. They’ll explain how to care for your new ostomy. They’ll also give you the supplies you’ll need to take care of it.
You’ll be able to go home once you:
You may have a home health nurse who will come to your home to help you with your ostomy.
Your team will understand that you’re receiving a lot of information soon after surgery. You may want to ask a family member or friend to sit in on these information sessions. Don’t hesitate to ask questions or ask your team to repeat any of the steps they’ve shown you.
It takes time to recover from abdominoperineal resection. You’ll continue to eat soft food for several weeks. If you work, it may be a few weeks before you can return. But your return to work depends on how well your surgical wounds heal and the type of work that you do.
Advertisement
You’ll have to avoid some activities during your recovery, including:
You should make sure you feel confident that you can drive safely. This includes being able to quickly hit the brakes.
Contact your surgeon if you have the following issues:
An APR is a major surgery. It leads to major life changes. Take your time to understand what this surgery means for you. Your surgeon will understand that you want to be comfortable with your decision. They and your care team members will take time to explain procedure details and how an APR may affect you. Don’t hesitate to ask for more information about what you can expect.
Advertisement
Some conditions like rectal and colon cancer, Crohn’s disease and ulcerative colitis may require colorectal surgery. Cleveland Clinic has the expert care you need.

Last reviewed on 07/16/2025.
Learn more about the Health Library and our editorial process.