Parkinson’s disease is a progressive condition that affects movement. It often starts with tremors, stiffness or slowness. It happens when brain cells that make dopamine stop working over time. There’s no cure, but medications and therapies may help manage symptoms to improve daily life.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Parkinson’s disease is a progressive movement disorder that worsens over time. It happens when brain cells that make dopamine slowly stop working. Dopamine is a chemical that helps control movement.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Common symptoms include tremors, muscle stiffness, slow movement and balance problems. You might also have symptoms that don’t affect movement, like sleep problems, mood changes or depression.
The disease is common. About 90,000 people in the U.S. are diagnosed with it each year. And an estimated 1 to 1.5 million people live with the condition.
There’s no cure for Parkinson’s disease. But treatment may help manage symptoms.
There are two types:
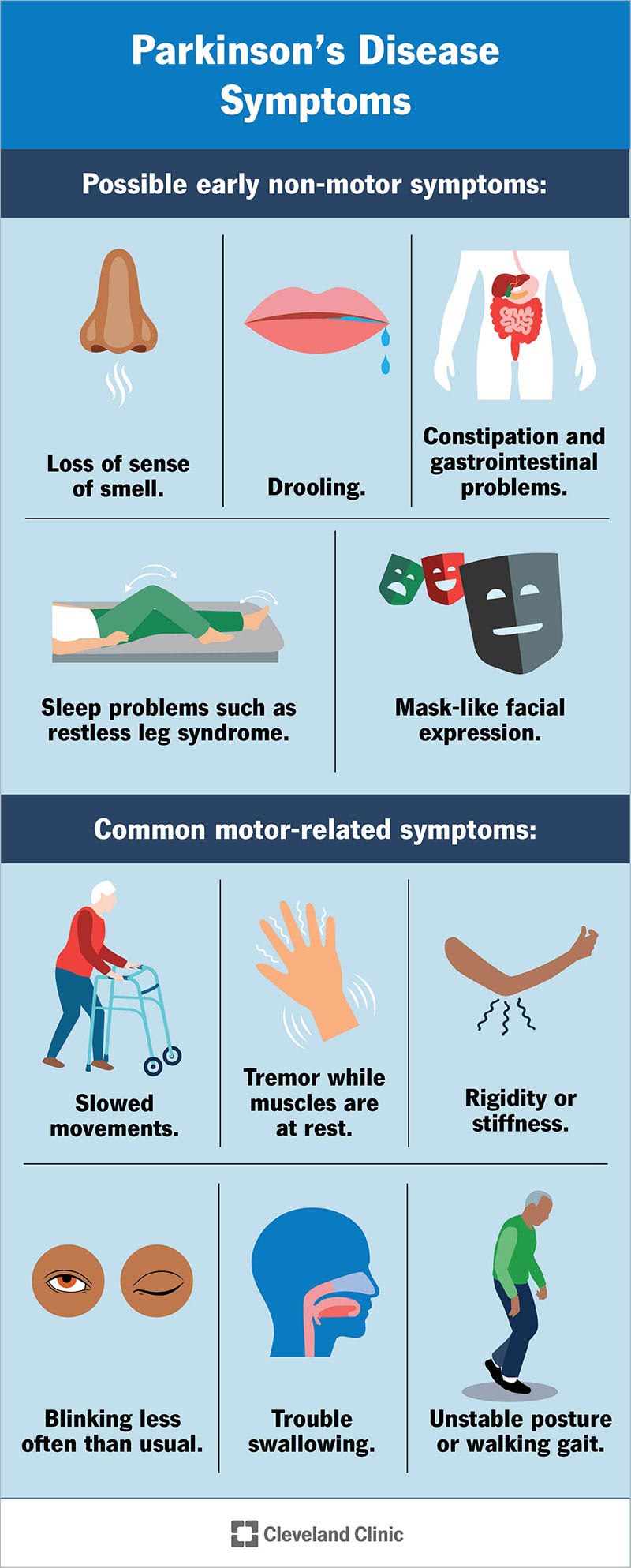
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/8525-parkinsons-disease)
Symptoms of Parkinson’s often start mild, slow and usually affect one side of your body first. Early symptoms may include tremors, stiffness or slower movement. Over time, these symptoms may affect both sides of your body and can make daily tasks harder.
Movement-related symptoms may include:
Advertisement
Non-movement symptoms may include:
Not everyone has the same symptoms. A healthcare provider can explain which symptoms are most likely and how they may change over time.
Parkinson’s disease happens when certain brain cells slowly stop working or die. These cells normally make dopamine. This is a chemical that helps with movement.
When dopamine levels drop, your brain has trouble sending signals to your muscles. This leads to symptoms like tremors, stiffness and slow movements. As the condition progresses, it can also affect thinking, mood and memory.
In many cases, the exact reason Parkinson’s disease develops still isn’t fully understood. For these reasons, there’s no way to prevent it.
You may be more likely to develop this condition if you:
The disease can lead to other health challenges over time. Common complications include:
These vary from person to person. A healthcare provider can watch for changes and offer support as your needs evolve.
Advertisement
Parkinson’s disease is mainly diagnosed through a medical exam and a discussion of symptoms. There isn’t one single test that can confirm it. Instead, healthcare providers look at how symptoms affect movement and how they change over time.
Your provider will start by reviewing your medical history and doing a neurological exam. They’ll watch how you move, walk and use your hands.
Tests help rule out other conditions. Your provider may recommend:
In some cases, genetic testing may help if Parkinson’s disease runs in your family. This isn’t common and is usually done only when there’s a strong family history.
Researchers are also studying newer lab tests that look for abnormal proteins linked to Parkinson’s disease. These tests aren’t widely used yet. But they may help with an earlier diagnosis in the future.
Treatment helps manage symptoms to improve daily life. Care usually involves a mix of medications, therapy and supportive care. Treatment plans are personalized and may change over time.
You can also ask your provider about clinical trials. These studies look at new ways to treat the condition.
Medications are the main treatment. They may replace or support dopamine, a brain chemical that controls movement. Providers may offer:
Advertisement
Several other medications treat specific symptoms, including:
These treatments deliver medication continuously under your skin through a pump. Options include foslevodopa and apomorphine. Providers typically consider them when symptoms like “on” and “off” periods continue despite oral medications. Choosing the right candidates, adjusting doses from pills to infusion and monitoring for side effects often requires care from a center experienced in advanced Parkinson’s treatments.
Advertisement
Therapies help you stay active and independent for as long as possible. These may include:
Surgery may be an option when medications no longer manage symptoms well. The most common type is deep brain stimulation (DBS). This implanted device helps reduce movement symptoms. But it’s not a cure, and it doesn’t stop the disease from progressing.
Healthy habits play an important role in managing this disease. Supportive care may include:
Working closely with a healthcare provider helps ensure your treatment matches changing needs over time.
You should consider seeing a healthcare provider if you notice:
If something feels off or starts getting in the way of your daily life, it’s OK to bring it up. Your provider can decide whether further testing or a referral to a specialist is needed.
Parkinson’s disease is a long-term condition that slowly gets worse over time. How fast it changes varies from person to person. Some people notice changes slowly over many years, while others may progress more quickly.
Treatment can help manage symptoms. You may need ongoing care and regular changes to your treatment plan. Living with Parkinson’s often means adjusting your routine and accepting support as needs change.
Parkinson’s disease isn’t usually fatal on its own. It’s a long-term condition that slowly gets worse.
Many people live with Parkinson’s disease for many years, especially with regular medical care and support. As symptoms progress, complications can develop. These may include problems with balance, swallowing and thinking. It can also affect automatic body functions, like blood pressure.
Because of these, you may have a shorter life expectancy than someone without the condition. How the disease affects lifespan varies widely and depends on factors like age at diagnosis, overall health and symptom management.
Parkinson’s disease can bring changes that feel slow at first, like a shaky hand and slower steps. Over time, these changes can build up and begin to touch many parts of your daily life. That’s why having the right care and support really matters.
While there’s no cure yet, treatments may make a meaningful difference. From medications and therapy to surgery and support groups, there are many ways to manage symptoms and maintain independence.
Living with Parkinson’s means learning to adjust. But it doesn’t mean giving up the things that bring you purpose and joy. With the right care and support, you can keep finding ways to move forward.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Shaky hands aren’t always because you’re tired or hungry. Cleveland Clinic brain experts can diagnose and treat your tremors and other Parkinson’s disease symptoms.
