Allergies happen when your immune system overreacts to something that’s usually not harmful — like pollen, pet dander and certain foods. Symptoms can include everything from sneezing and a runny nose to vomiting and difficulty breathing. If you can’t avoid allergens, there are some medications that might help reduce your symptoms.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
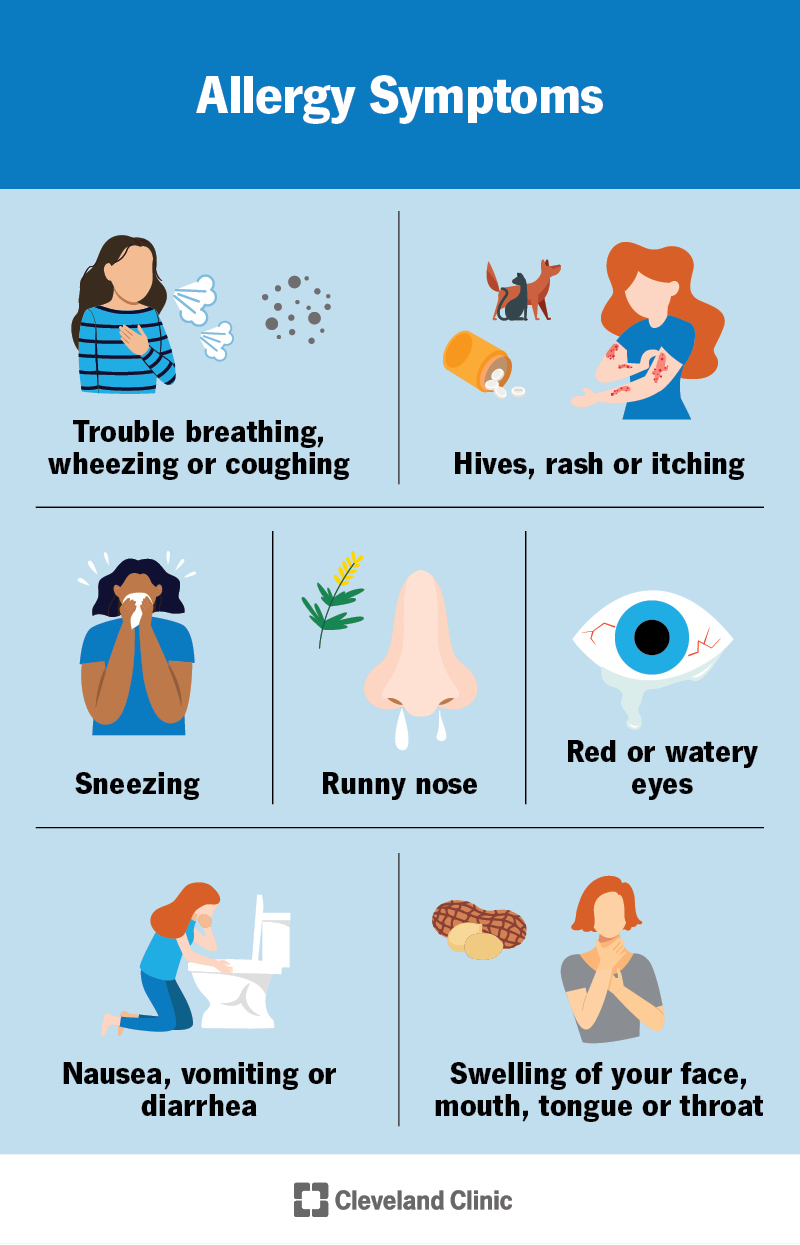
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/allergies-v2)
Allergies are your immune system’s overreaction to foreign substances. When you touch, inhale or eat something you’re allergic to, your body thinks it’s harmful and reacts to try to get rid of it. This can cause minor reactions like itching, sniffling and sneezing. But in some cases, allergic reactions can lead to life-threatening airway swelling and low blood pressure (anaphylaxis).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
You can be allergic to almost anything — like pollen, animals, medications and food. Some people have allergies that are merely annoying. Others have to completely alter their lives to avoid reactions.
Some common allergies include:
Allergies can cause a range of symptoms, including:
Symptoms often depend on how you’re exposed to an allergen. For instance, if you touch something you’re allergic to, you might get an itchy rash. If you’re allergic to pollen or pet dander, you usually get a runny nose or sneeze when you breathe them in. Food and drug allergies and bee stings are more likely to cause severe reactions, like airway swelling and vomiting.
Your allergies will continue as long as you’re exposed to the allergen. Some start within minutes of exposure, while others don’t start until hours or days later. Once you’re no longer around allergens, your symptoms should go away after a few hours. Some allergies, like poison ivy rashes, can last for a few weeks.
Advertisement
Allergies happen when your immune system mistakenly identifies foreign proteins — in pollen, pet dander, medications, food or other substances — as something harmful (as if it were a virus or bacteria). Inhaling, eating or touching something you’re allergic to activates mechanisms meant to protect you and flush the allergen out of your system. This causes your symptoms, which can sometimes be life-threatening.
You generally have to be exposed to a substance more than once before you’ll react to it. The first time you’re exposed, your body sees it as foreign and creates antibodies to it (sensitization). The next time you’re exposed to the same substance, it activates the antibodies. This alerts your immune system to attack, triggering your symptoms.
You’re more likely to have allergies if you have:
A healthcare provider can diagnose allergies with a skin test or blood tests. To determine what allergens to test for, they’ll ask you about your symptoms and any possible allergens you could be exposed to, like through work or hobbies.
Depending on your suspected allergies, they might also recommend breathing tests, drug or food challenge tests, or a patch test. A patch test looks for a contact skin reaction that happens over a few days.
Avoiding things you’re allergic to is your best bet to manage allergies. This is especially true if your allergies are likely to cause anaphylaxis.
But some common allergens can be hard to avoid. Your healthcare provider might recommend you take certain medications daily or get specific treatments regularly. These can reduce your symptoms or risk of a reaction. Depending on your allergies, options could include:
If you have an allergy that could cause a severe reaction, your provider will recommend you carry an epinephrine auto-injector (EpiPen® or Auvi-Q®) to use at the first signs of a severe allergic reaction.
Talk to a healthcare provider if you have symptoms of allergies and want to get to the bottom of what’s causing them. A primary care provider might refer you to a specialist, like an allergist or dermatologist, to get certain tests.
Go to the ER or call 911 if you experience:
Advertisement
What to expect when you have allergies depends on what kind they are. Seasonal or pet allergies are generally more likely to cause irritating, but not life-threatening, reactions. Food and drug allergies and bee stings are more likely to cause serious reactions. You’ll probably need to carry an epinephrine injector if you have one of these allergies.
If you’re still having bothersome allergy symptoms even with treatment, you might get some relief with:
You can’t really avoid developing allergies to begin with. To avoid reactions to known allergens, you can:
Advertisement
If you have a food allergy, check food labels, keep allergen-free foods in your house, and only eat at restaurants where you know you can eat something that’s allergen-free.
Allergies can change with age. This can depend on how much (or how little) you’re exposed to an allergen, changes in your immune system and other factors.
Sometimes, existing allergies get worse, or allergies that seemed to have gone away can come back. Other times, existing allergies can get better over time — say, if you’re allergic to cats but you’re around them regularly anyway. Finally, some people can get new allergies as adults.
Allergies are a part of everyday life for millions of people around the world. If you’re not sniffling and sneezing every spring, you’re trying to avoid the rash you’ll get from your neighbor’s overly affectionate dog. Food and drug allergies are often more serious — they mean carefully reading labels and being cautious about new medications. But for most, allergies are manageable. Talk to your healthcare provider about any concerns you have.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Allergies can wreak havoc on your life. At Cleveland Clinic, our team of experts can help create a treatment plan that’ll help you breathe easier.
