Overview
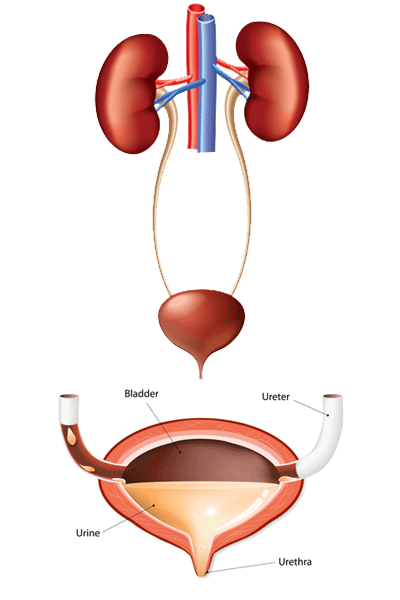
The bladder is a hollow organ in the pelvis, which acts as a reservoir for urine until it is eliminated from the body through urination.
The bladder has flexible, muscular walls that can expand and contract with the volume of urine. The walls consist of four main layers: an inner lining of urothelial or transitional cells; a thin layer of connective tissue, blood vessels and nerves; a thick layer of muscle; and an outer layer of fatty tissue.
Bladder cancer is a disease in which an uncontrolled growth of abnormal (tumor) cells arise in these tissues. Bladder cancers usually start from the inner lining (urothelium) of the bladder. Cancer cells can then develop the ability to penetrate the layers of the bladder wall. The deeper the penetration, the more likely the cancer cells have spread to the blood stream or lymph nodes surrounding the bladder and other organs.
Cleveland Clinic urologists treat all types of bladder cancer and tailor bladder cancer treatment plans to their patients’ needs. This guide provides an overview of the bladder cancer treatment options offered at Cleveland Clinic.
How is bladder cancer diagnosed?
At Cleveland Clinic we use several tests and procedures to diagnose bladder cancer. These include a medical history, physical exam, urinalysis and urine cytology, which is a laboratory test to check for abnormal cells in your urine. A CT scan or MRI can determine whether the cancer has spread to any other locations in your body.
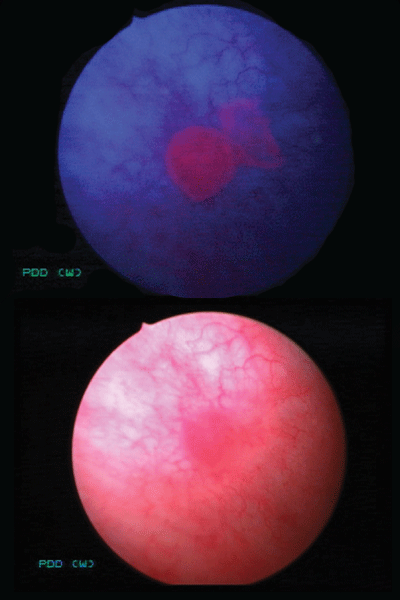
Our urologists almost always perform a cystoscopy; it allows us to look inside the bladder and urethra with a thin tube-like instrument with a camera (a cystoscope) to look for abnormalities and remove tissue samples. Cysview® blue light cystoscopy is also sometimes used. This technique uses a fluorescent dye to highlight tumors when the bladder is illuminated with a special light. During the procedure we examine the bladder in blue light. The dye accumulates in any abnormal cells and glows pink under the blue light, highlighting the cells’ location against normal bladder tissue. This technology improves our ability to detect cancers that might otherwise be missed.
Stages of Bladder Cancer
Bladder tumors are characterized by type, stage and grade. This characterization helps us to determine both the therapy that is most likely to be successful and how many people survive 5 years with a particular stage and grade of bladder cancer.
Several staging systems exist for bladder cancer. The most common is the TNM system in which T = tumor, N = nearby lymph node involvement and M = metastasis (or spread to locations outside of the bladder). Each letter is followed by a number to indicate the extent of the primary tumor and the degree of spread. Another staging system categorizes tumors as stage I to IV.
Grade refers to how closely a cancer cell looks like a normal cell under the microscope. There are two main grades: low grade and high grade. Low-grade cancers have well-differentiated cells and look similar to normal cells that form the inner lining of the bladder, but they can return after they are removed. High-grade cells, on the other hand, are very disorganized, look quite different and distorted, and vary greatly in size, compared with normal cells. High-grade cells make up the most aggressive form of bladder cancer. They not only can recur after they are removed, but they also have the biologic potential to invade deeper into the bladder wall and spread to other parts of the body.
In addition to staging, your doctor will perform a number of diagnostic studies such as biopsies and CT scans or MRI’s to answer three main questions:
- Tumor (T): How deep has the cancer invaded the bladder wall? Has it invaded organs that are next to the bladder such as the prostate?
- Node (N): Do any lymph nodes in the pelvis contain cancer cells? If so, how many?
- Metastasis (M): Has the cancer spread to other organs? If so, where and how many spots?
We then combine the cancer’s TNM information to assign an overall stage, which will be used for counseling and treatment decisions:
- Stage 0a: Early cancer that has formed a papillary (cauliflower-like) growth that is confined to the lining of the bladder and has not invaded the connective tissue or muscle of the bladder wall.
- Stage 0is: Flat tumor or carcinoma in situ (CIS) involving the lining of the bladder. These cancers are always high grade, can be difficult to detect and behave aggressively by invading the bladder wall if not treated.
- Stage I: The cancer has invaded the lamina propria or first connective tissue layer of the bladder.
- Stage II: The cancer has invaded through the lamina propria and into the muscle layer of the bladder.
- Stage III: The cancer has invaded through both the lamina propria and muscle layer and outside the bladder into the fatty tissue layer that surrounds the bladder, organs that are adjacent to the bladder such as the prostate in men or vagina in women, or spread into the lymph nodes surrounding the bladder.
- Stage IV: The cancer has invaded the pelvic or abdominal wall, spread to distant lymph nodes, or spread to distant organs such as the lungs, liver or bones.
What causes bladder cancer?
Bladder cancer is usually caused by prolonged exposure to a carcinogen (cancer-causing chemical). Carcinogens are filtered by the kidney into the urine. These carcinogens then can damage the inner lining of the bladder as they sit in the urine against the cells’ surface until urination is possible.
The greatest risk factor for bladder cancer is cigarette smoke, which causes 60% of all bladder cancers. If you smoke, your risk of developing bladder cancer is two to six times that of a nonsmoker. Occupational and environmental carcinogens can also cause bladder cancer; for example, exposure to aromatic amines may contribute to increased bladder cancer risk in people who work in the rubber, leather, textiles and paint product industries. Firefighters may have an increased bladder cancer risk from regular exposure to chemical fumes and smoke. Drinking water from wells contaminated with arsenic is also linked to increased bladder cancer risk. Sometimes it takes many years from the exposure to actually develop bladder cancer.
Bladder cancer risk increases with age; it is rarely diagnosed in patients under 40 years of age. Men are at least three times more likely than women to get bladder cancer, but women with bladder cancer may delay seeking treatment, because many bladder cancer signs and symptoms mimic those of other urinary and gynecologic diseases. Caucasians get bladder cancer more often than African Americans. Asians have the lowest risk.
Other risk factors include:
- Previous radiation exposure to the pelvic area, for example, during treatment for prostate or cervical cancer.
- Certain chemotherapy drugs, such as cyclophoshamide.
- A previous diagnosis of bladder cancer. (Bladder cancer has a 50% to 80% chance of recurrence.)
What are the warning signs of bladder cancer?
Blood in the urine (hematuria)is the most common and important warning sign. Hematuria can be classified as gross (visible to the naked eye) or microscopic (only seen with a microscope). Gross hematuria is much more likely to be associated with bladder cancer than microscopic hematuria, but blood in the urine should never be ignored since hematuria is usually painless and intermittent when caused by bladder cancer.
Other symptoms of bladder cancer include a change in bladder habits such as an unexplained increase in urinary frequency and urgency. Some patients will present with pain or burning during urination. Symptoms of advanced bladder cancer include an inability to pass urine, pain in the flank caused by obstruction of urine flowing from the kidney to the bladder, rapid weight loss, appetite loss, increased fatigue, and unremitting pelvic pain and/or bone pain.
Grading Bladder Cancer
Pathologists “grade” the cancer according to the nature of the cancer cells within the tissue samples they have received from biopsies and examined under a microscope. There are two main grades: low-grade, or well-differentiated cells, and high-grade, or poorly differentiated cells. Lowgrade cells may vary in size but most look relatively normal under magnification. High-grade cells, which make up the most aggressive form of bladder cancer, appear distorted and vary greatly in size. Whether tumors are low- or highgrade, they can recur throughout the urinary tract. Highgrade tumors may also spread to other parts of the body by invading lymphatic channels or blood vessels.
Types
What are the different types of bladder cancer?
There are several types of bladder cancer. Each can be defined by:
- What the cancer cells look like under magnification.
- Where in the bladder the cancer cells originate, the types of cells that are involved, and where and how they grow.
- How far the cancer cells have penetrated the bladder’s multi-layered wall. Non-invasive bladder cancers remain in the innermost, transitional epithelium layer. Invasive cancers grow into the adjacent layer of connective tissue, blood vessels and nerves, or even farther into the muscle layer. Invasive cancers are more likely to spread and are harder to treat.
Transitional cell (urothelial) carcinoma occurs in the cells that line the bladder’s interior and other parts of the body’s urine-handling system — the renal pelvis (a funnel-like structure in each kidney), the ureters (tubes that connect the kidneys to the bladder), and the urethra (the tube that carries urine outside the body).
Transitional cell carcinoma is the most common type of bladder cancer, making up more than 90 percent of all cases. There are two subtypes:
- Papillary urothelial tumors are thin, cauliflower-like projections that sprout from the bladder’s inner lining and grow toward the organ’s hollow center. Very-lowgrade, non-invasive papillary urothelial carcinomas (also called low-malignant-potential tumors) don’t penetrate into deeper bladder wall layers and are unlikely to spread elsewhere in the body. Malignant papillary carcinomas are more common. The low-grade variety seldom invades farther into the bladder wall but is likely to recur after surgical removal. High-grade papillary carcinomas are more prone to be invasive and to recur in the bladder or elsewhere in the urinary tract. Patients who have had bladder tumors removed are examined regularly to check for recurrence.
- Flat urothelial carcinomas also originate in the bladder’s inner lining but don’t produce stalks like papillary urothelial carcinomas. If the abnormal cellular growth is limited to the inner lining, the condition is called carcinoma in situ (CIS). Flat urothelial CIS is classified as high-grade, meaning it is aggressive and has the potential to recur following removal and to invade other layers of the bladder wall and spread elsewhere in the body.
Several other types of bladder cancer are much less common than transitional cell carcinoma and involve other types of cells. Each is aggressive and can be difficult to treat. They include:
- Squamous cell carcinoma, which begins in thin, flat, skin-like cells that appear in the bladder’s inner lining in response to infection or inflammation.
- Adenocarcinoma, which can arise in any part of the bladder or spread from elsewhere.
- Small cell carcinoma, which occurs in nerve-like cells of the bladder called neuroendocrine cells.
- Sarcoma, which starts in the bladder’s muscle cells.
Treatments
What are the treatment options for bladder cancer?
Treatment for bladder cancer depends on several factors, including stage (the tumor’s location and extent), grade (the cancer’s aggressiveness and potential for spread), and your age and general health. The four types of treatment for patients with bladder cancer include:
- Surgery.
- Intravesical therapy (immunotherapy or chemotherapy placed into the bladder through a catheter).
- Systemic therapy (including chemotherapy, immunotherapy and other drugs given through the veins).
- Radiation therapy.
Sometimes combinations of these treatments are used to improve cancer control.
Surgery
Surgery is the most common treatment option and generally the first option for bladder cancer. The type of surgery chosen will depend on the stage of the cancer.
- Transurethral resection of bladder tumor (TURBT) is used most often for the initial diagnosis of bladder cancer and the treatment of early stage disease (non-invasive – stage 0 or non-muscle invasive – stage 1). It is usually done under general anesthesia. In this procedure, a cystoscope is inserted into the urethra and advanced into the bladder, and no incisions are made. Miniaturized surgical instruments are threaded through the cystoscope to remove the tumor and any other areas that appear suspicious. After surgery some blood in the urine and discomfort may occur. Most patients return home the same or the following day and resume normal activities in less than one week. A Foley catheter may be placed after the procedure to drain urine while the bladder is healing
- Radical cystectomy is used if your cancer has invaded the muscle layer, involves other organs that are close by, spread to the local lymph nodes or cannot be controlled by TURBT and intravesical Bacillus Calmette-Guérin (BCG). Before surgery is performed, you will undergo CT and/or MRI to confirm that the cancer has not spread to a distant site. The surgery involves removing the bladder, adjacent organs and lymph nodes that are in the pelvis. Your surgeon then reconstructs the urinary tract in one of three ways:
- Ileal conduit uses a short piece of small intestine and is the simplest and most common way to divert the urine. The urine drains continuously into this piece of small intestine that is connected to the skin on the right side of the body near the belly button. A bag placed over the stoma (opening) collects urine. Care of the ileal conduit involves emptying the bag whenever it is full and changing the bag every few days
- Continent cutaneous diversion uses a piece of small and large intestine to shape a pouch that is connected to the skin via a thin, catheterizable channel. No external bag is needed to collect urine, but you will need to empty the pouch of urine with a catheter every few hours.
- Neobladder uses a long piece of small intestine to shape a pouch that is connected to the urethra, so that urine is eliminated from the body in a more normal fashion. Since the neobladder is not connected to your brain the same way your bladder is, you will have to re-learn how to urinate.
Not all of these urinary diversions are options for every patient, and each has its own advantages and disadvantages. You will need to talk with your urologist to decide the best option for you. Cleveland Clinic surgeons are well experienced in robotic and open radical cystectomy, and the approach is individualized to each patient.
- Partial cystectomy is the removal of only the portion of the bladder with cancer. It is not commonly performed but may be an option if you have muscle-invasive tumors limited to one part of the bladder. Removing that part of the bladder leaves you with enough functional bladder capacity to urinate normally.
Intravesical therapy
Intravesical therapy involves instilling medications directly into the bladder and is used after TURBT in patients with cancer that has not invaded the muscle layer. Its purpose is to prevent the cancer from coming back or invading deeper into the wall. The exact type of medication depends on cancer grade and stage. Some patients may receive intravesical chemotherapy immediately after surgery (Mitomycin-C or gemcitabine) or as a 6- or 8-week course starting approximately 4 weeks after surgery. Since the chemotherapy remains in the bladder, you will not have any of the usual side effects associated with chemotherapy that is given into the veins, such as getting sick to your stomach or losing your hair.
- The mainstay of treatment for high-grade bladder cancers that have not invaded the muscle is intravesical Bacillus Calmette-Guérin (BCG), one of the first immunotherapies developed for cancer. BCG is a live, weakened bacteria (mycobacterium) that stimulates the immune system to attack bladder cancer cells. Treatment starts several weeks after TURBT and involves placing a catheter into the bladder, draining the bladder of urine, instilling BCG into the bladder and removing the catheter. You will need to hold the BCG for as long as possible - up to 2 hours. If BCG treatment is successful, you may be asked to undergo maintenance BCG therapy, which includes three doses every 6 months and can last up to 3 years. Common side effects of BCG treatment include more frequent urination, painful urination, low grade fever, or flu-like symptoms such as muscle/joint pains or chills. Your urologist will schedule a cystoscopy approximately 6 weeks after the last BCG instillation to evaluate the effectiveness of treatment.
- A newer intravesical immunotherapy option called nadofaragene firadenovec. This treatment is a gene therapy that uses the natural protein-making machinery of the urothelial cells to stimulate the production of a protein called interferon alfa-2b, which in turn stimulates the immune system to fight the cancer.
Systemic therapy
Systemic therapy involves administering drugs through your veins to control the bladder cancer. These drugs are given by medical oncologists who are part of your treatment team.
- Chemotherapy. The most common form of systemic therapy is chemotherapy, which works by killing rapidly dividing cells. Chemotherapy affects cancer cells more than normal cells, because cancer cells divide more quickly. In some patients with muscle-invasive bladder cancer, chemotherapy is given before radical cystectomy (called neoadjuvant therapy), because clinical trials have demonstrated that doing so will improve survival. Adjuvant chemotherapy is the administration of chemotherapy after surgery, which is sometimes done if the pathology results show that the cancer is more advanced (e.g., spread to pelvic lymph nodes) than expected.
- Immunotherapy is another type of systemic therapy that activates the immune system to fight bladder cancer. The most commonly used immunotherapy in bladder cancer is intravesical BCG. More recently a systemic immunotherapy called checkpoint inhibitors, has been developed to treat bladder cancer. Cancer cells can prevent attack by the immune system by making a protein called PD-L1. PD-L1 binds to PD-1, a protein found on the surface of T-cells (a type of immune cell) that keeps the immune system at bay. Checkpoint inhibitors stop PD-L1 from interacting with PD-1, which allows the immune system to recognize and attack cancer cells.
- Antibody drug conjugates (ADC) are complex molecules that combine two distinct parts (enfortumab vedotin). One part is a monoclonal antibody, which is a Y-shaped molecule that recognizes and binds tightly to a protein on a cancer cell’s surface. The other part is a highly toxic drug that destroys cancer cells. These two parts are joined by a linker. ADCs function like a smart bomb by targeting cancer cells with the antibody component and releasing its payload to cause cell death.
Radiation therapy
Radiation therapy damages the DNA of cancer cells by bombarding them with high-energy X-rays or other types of radiation. The radiation source is a machine outside the body that directs a focused beam of radiation at the tumor. Computer-guided radiation delivered from several angles minimizes radiation exposure to surrounding tissues and organs, limiting damage to these tissues. Common side effects of bladder radiation include fatigue, skin irritation such as redness, blistering, and peeling, bladder symptoms such as pain during urination, increased urgency, incontinence and bloody urine.
Trimodality therapy (TMT) may be an option for a small number of patients with muscle-invasive bladder cancer who do not have bothersome urinary symptoms, have a solitary tumor without CIS, are strongly motivated to keep their bladder or cannot tolerate radical cystectomy. After undergoing aggressive TURBT to eliminate all visible tumor in the bladder, you receive a combination of chemotherapy and radiation, which is given for several weeks after surgery. After treatment, you are followed closely with cystoscopy and CT or MRI scans for cancer detection. Some patients have an incomplete response to this treatment or have the cancer recur in the muscle layer of the bladder, in which case surgeons may recommend salvage cystectomy for cancer control.
Prognosis
Your chances of cure depend on several factors. These are:
- The stage of your cancer (whether it is superficial or invasive) and whether it has spread to other places in your body. Early stage bladder cancer can often be cured. If you have non-muscle-invading bladder tumors, you should have periodic cystoscopy exams to monitor your condition. How often the exams are done depends on the grade and stage of your tumor(s) and how often they recur.
- The type of cancer cells (high grade or low grade) and how abnormal they look under the microscope.
- Your age and general health.
Prognosis can also depend on how many tumors there are, their size and whether they have recurred or spread after treatment.
Clinical Trials
You may be eligible to participate in a clinical trial at Cleveland Clinic. We depend on these trials to determine whether a new treatment or approach is better than existing treatments or has fewer side effects. Please discuss with your surgeon whether a clinical trial may be appropriate for you.
Support Services
Making Your Care Easier
The life-changing events that occur when you or a loved one is diagnosed with cancer are challenging. Cleveland Clinic Cancer Center offers many services and programs to help you navigate those changes while promoting your well-being. Services include the 4th Angel Mentoring Program, educational resources, psycho-social programs, support groups, financial services, free wigs and a variety of wellness programs.
Medical Concierge
If you are traveling from out of state and need assistance, call our complimentary Medical Concierge at 800.223.2273, ext. 55580, or email medicalconcierge@ccf.org.
Global Patient Services
Complimentary assistance for international patients and families is available by phone at 001.216.444.8184, or by visiting our Global Patient Services page.
MyChart
Cleveland Clinic MyChart® is a secure, online personal healthcare management tool that connects patients to portions of their medical record at any time, day or night. Patients can view test results, renew prescriptions, review past appointments and request new ones. Patients may register for MyChart through their physician’s office or online.
Appointments & Locations
Appointments
Cleveland Clinic Cancer Center provides patients with convenient locations throughout Northern Ohio for screening and treatment of bladder cancer. In addition to Cleveland Clinic’s main campus, patients can visit Cleveland Clinic regional hospitals and family health centers. Every member of our bladder cancer treatment team is committed to providing you with outstanding, comprehensive, efficient and compassionate care. To find a cancer specialist near you, call 866.223.8100.
Locations
Cleveland Clinic Cancer Specialists are located in Cleveland, regionally throughout Northern Ohio and in Florida. View a complete list of cancer care locations.
Virtual Second Opinion
If you cannot travel to Cleveland Clinic, help is available. You can connect with Cleveland Clinic specialists from any location in the world via a phone, tablet, or computer, eliminating the burden of travel time and other obstacles. If you’re facing a significant medical condition or treatment such as surgery, this program provides virtual access to a Cleveland Clinic physician who will review the diagnosis and treatment plan. Following a comprehensive evaluation of medical records and labs, you’ll receive an educational second opinion from an expert in their medical condition covering diagnosis, treatment options or alternatives as well as recommendations regarding future therapeutic considerations. You’ll also have the unique opportunity to speak with the physician expert directly to address questions or concerns.
Why Choose Us?
For many types of cancer there are significant differences in outcomes among treatment centers. Cleveland Clinic makes its treatment outcomes available for the public. Research shows that medical institutions with experience caring for large numbers of patients have better outcomes. Cleveland Clinic Cancer Center treats tens of thousands of patients each year. Also, Cleveland Clinic Cancer Center patients are likely to experience shorter hospital stays, fewer complications, better management of side effects and access to new therapies through clinical trials.
A New Home for Cancer Care
When you visit Taussig Cancer Center, Cleveland Clinic’s new $276 million, 377,000-square-foot home for cancer care, some of its features are immediately apparent: expansive, welcoming spaces, the abundance of natural light, and the combination of clinical care and support services. A deeper look reveals a facility designed expressly to improve patient outcomes through a collaborative, multidisciplinary approach to cancer care. The new cancer building on Cleveland Clinic’s main campus, with 126 exam rooms and 98 treatment rooms, incorporates all outpatient cancer services under one roof. The building creates a seamless, personalized experience for patients and provides easy access to a variety of support services intended to reduce cancer’s psychological stress.
