Overview
What is the Pericardium?
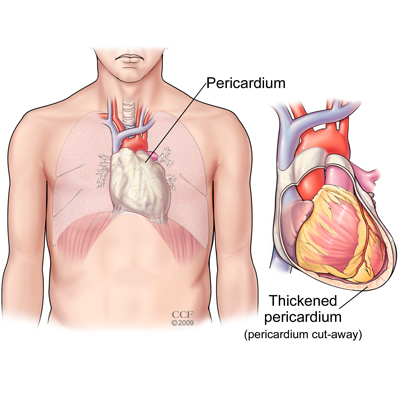
The pericardium is a thin, two-layered, fluid-filled sac that covers the outer surface of the heart. It shields the heart from infection or malignancy and contains the heart in the chest wall. It also prevents the heart from over-expanding when blood volume increases, which keeps the heart functioning efficiently.
What is Pericarditis?
Pericarditis is an inflammation of the pericardium. Pericarditis is usually acute – it develops suddenly and may last up to several months. If you could see and touch it, the membrane around the heart would look red and swollen, like the skin around a cut that becomes inflamed. Sometimes excess fluid develops in the space between the pericardial layers and causes a pericardial effusion (buildup of excess fluid around the heart). Recurrent pericarditis is diagnosed if symptoms improve for 4-6 weeks and then recurs. Incessant pericarditis occurs when the symptoms continue non-stop for 12 weeks.
Who gets pericarditis?
Most cases of pericarditis occur in men aged 20 to 50, although pericarditis also can occur in women.
When To See A Doctor
If you have any of the symptoms of acute pericarditis, you should schedule an exam with your doctor immediately. Left untreated, pericarditis can become a life-threatening condition because pericardial effusion can develop and possibly lead to cardiac tamponade (a severe compression of the heart that impairs its ability to function).
Symptoms of cardiac tamponade include chest pain, difficulty breathing, fainting, light-headedness, palpitations or rapid breathing. These symptoms require emergent treatment; call 911 if you experience any of these symptoms.
If you develop symptoms of constrictive pericarditis (thickening or scarring of the pericardium), including shortness of breath, swelling of the legs and feet, water retention, heart palpitations, and severe swelling of the abdomen, you should make an appointment with your cardiologist for an evaluation.
Symptoms
Chest pain symptoms associated with pericarditis can be described as:
- Sharp and stabbing (caused by the heart rubbing against the pericardium)
- May increase with coughing, swallowing, deep breathing or lying flat
- Can be relieved by sitting up and leaning forward
You also may feel the need to bend over or hold your chest to breathe more comfortably.
Other symptoms include:
- Pain in the back, neck or left shoulder
- Difficulty breathing when lying down
- A dry cough
- Anxiety or fatigue
In some people, pericarditis can cause swelling of the feet, legs or ankles. This swelling may be a symptom of constrictive pericarditis, a serious type of pericarditis. In constrictive pericarditis, the patient’s pericardium hardens and/or thickens, preventing the heart muscle from expanding and affecting the function of the heart. The heart may be compressed by the constrictive process, which may cause blood to back up into the lungs, abdomen and legs, as well as cause the swelling.
If you have any symptoms of acute pericarditis, it is important to call your doctor right away.
If you feel your symptoms are a medical emergency, do not wait for an appointment. Call 911 immediately and ask to be transported to the nearest hospital.
Causes
There are many causes of pericarditis, but it is often a complication of a viral infection (viral pericarditis) – usually a gastrointestinal virus, or rarely the flu virus or AIDS. It may also be caused by a bacterial infection (bacterial pericarditis), fungal infection (fungal pericarditis) or parasitic infection (parasitic pericarditis). A more recent cause can be the Covid-19 infection.
Certain autoimmune diseases, such as lupus, rheumatoid arthritis and scleroderma, also can cause pericarditis. Additional causes of pericarditis include injury to the chest such as after a car accident (traumatic pericarditis), other health problems such as kidney failure (uremic pericarditis), tumors, genetic diseases such as Familial Mediterranean Fever (FMF), or rarely, medications that suppress the immune system.
The risk of pericarditis is greater after a heart attack or after heart surgery (Dressler’s syndrome), radiation therapy or a percutaneous treatment, such as cardiac catheterization, radiofrequency ablation (RFA) or pacemaker implantation.
Diagnosis
You doctor will start with an evaluation of your symptoms: the sharp pain in the chest and back of the shoulders, and difficulty breathing are two major clues that you may have pericarditis rather than a heart attack. Your doctor also will ask you about your medical history, such as whether you have had a recent viral illness. He or she should already know about any previous heart surgery or current diseases, such as lupus or kidney failure, that may increase your risk of pericarditis.
During a physical exam, the doctor will listen to your heart with a stethoscope. Pericarditis may cause a rubbing or creaking sound, called the “pericardial rub,” that is produced by the rubbing of the inflamed lining of the pericardium. This is best heard when the patient leans forward while holding his or her breath, and when breathing out. Depending on how severe the inflammation is, your doctor may also hear crackles in the lungs, signs of fluid in the space around the lungs, or excess fluid in the pericardium.
Cleveland Clinic imaging specialists in the Center for the Diagnosis and Treatment of Pericardial Diseases often use a multifaceted approach to diagnose pericarditis and identify complications related to the condition, such as pericardial effusion and constrictive pericarditis. Some of the tests we use include:
- Chest X-ray: To look for enlargement of the heart and fluid build-up in the lungs.
- Electrocardiogram (ECG/EKG): Pericarditis causes changes in your heart rhythm. An ECG records your heart’s electrical activity. Two problems related to pericarditis are diffuse ST elevation, which indicates electrical problems in the bottom chambers of the heart (ventricles) and PR depression, which is related to electrical issues in the top chambers of the heart (atria).
- Echocardiogram (echo): Uses ultrasound to check the heart for problems such as fluid build-up in the pericardium (pericardial effusion) and a stiff, thick pericardium (constrictive pericarditis).
- Cardiac MRI and CT scan: Show excess fluid in the pericardium or signs of pericardial edema and inflammation using a special imaging agent called gadolinium. These tests may also show a thickened pericardium or compression of the heart from the thickening.
- Cardiac catheterization: Provides hemodynamic information about the filling pressures within the heart in order to confirm a diagnosis of constrictive pericarditis. The pressures are elevated and equal across all the four chambers of the heart.
- Laboratory (blood) tests: Can be used to make sure you are not having a heart attack, to evaluate the heart’s function, test the fluid in the pericardium and determine the underlying cause of the pericarditis. Often, the sedimentation rate (ESR) or C reactive protein levels or high sensitivity C reactive protein (markers of inflammation) and white blood count (WBC) are elevated. Other laboratory tests such as anti-nuclear antibodies (ANA), rheumatoid factor (RF) are for evaluation for autoimmune diseases.
Treatments
Treatment for acute pericarditis (sudden onset) may include medication for pain and inflammation, such as nonsteroidal anti-inflammatory drugs, including ibuprofen or aspirin in large doses. Depending on the cause of your pericarditis, your doctor may prescribe an antibiotic (for bacterial pericarditis) or an antifungal medication (for fungal pericarditis).
If your symptoms last longer than two weeks or recur over subsequent months, your doctor may prescribe an anti-inflammatory drug called colchicine in combination with the ibuprofen (first line therapy). Colchicine is an older and well established anti-inflammatory drug that can help control the inflammation and prevent pericarditis from recurring weeks or even months later.
When high doses of ibuprofen are prescribed, your doctor may prescribe medications called proton pump inhibitors to offset gastrointestinal symptoms. If you are taking high doses of nonsteroidal anti-inflammatory drugs, you should be monitored with frequent follow-up appointments to evaluate changes in kidney or liver function. Second line therapy includes low dose prednisone with a low taper. Third line therapy includes IVIG, interleukin receptor antagonists, methotrexate or azathioprine. Fourth line therapy includes radical pericardiectomy.
Between 15% to 30% will develop recurrent pericarditis after the first episode. This is defined as a return of symptoms after four to six weeks of improvement or incessant pericarditis that is symptoms continuous for three months. Chronic pericarditis is defined as symptoms after three months. These patients may need to take nonsteroidal anti-inflammatory drugs or colchicine for several years, even when they are feeling well. Previous treatment included the use of steroids, such as prednisone; however, this has been found in many cases to cause dependency on the medication to prevent a return of symptoms. In addition, steroids can reactivate the original viral infection. Furthermore, some patients can become dependent on narcotics for pain control. For patients experiencing a lot of pericardial inflammation, some newer studies have suggested interleukin receptor antagonists can be included as part of second line therapy.
Are Procedures Needed to Treat Pericarditis?
For most people with pericarditis, treatment with medications is all that is needed to clear up the inflammation and surgery is not usually necessary.
Sometimes fluid builds up in the pericardium, causing the heart to be compressed. If this occurs, you may need to undergo pericardiocentesis – a procedure to drain the excess fluid with a catheter. The doctor will use echocardiography to safely guide the placement of a large needle and catheter into the pericardium to remove excess fluid. If the fluid cannot be drained with a needle, then a surgical procedure called a pericardial window is performed.
Surgery may be needed for some patients with constrictive pericarditis. Complete or radical pericardiectomy is the surgical treatment of pericarditis that involves the removal of the whole pericardium. Surgery is rarely done for pain control of recurrent pericarditis.
Complications
Constrictive Pericarditis
Constrictive pericarditis is a severe form of chronic pericarditis in which the inflamed layers of the pericardium stiffen, develop scar tissue, thicken and stick together. The thick, rigid pericardium constricts the heart’s normal movement so that it cannot expand normally as it fills with blood. As a result, the heart chambers don’t fill up with enough blood. The blood then backs up behind the heart, causing symptoms of heart failure, including shortness of breath, swelling of the legs and feet, water retention and disturbances in the heart’s normal rhythm. These symptoms should improve when the constrictive pericarditis is treated.
Constrictive pericarditis often can be treated with a diuretic, such as furosemide, to treat the fluid retention. If you develop a heart rhythm problem, you may need to take a medication to treat the irregular rhythm for as long as the constrictive pericarditis lasts or until your heart rhythm returns to normal. When none of these treatments are effective, pericardiectomy may be needed to surgically remove the stiffened pericardium.
Pericardial Effusion
When an excess of fluid builds up in the space between the pericardium, it can cause a condition known as pericardial effusion. Rapid fluid accumulation in the pericardium can cause cardiac tamponade, a severe compression of the heart that impairs its ability to function. Cardiac tamponade resulting from a pericardial effusion can be lifethreatening and is a medical emergency requiring emergent drainage of the fluid with a catheter.
Outlook
What is the outlook after pericarditis?
In most people, pericarditis persists for up to three months then goes away and does not come back. If it does not go away, then it becomes complicated pericarditis.
After you recover from the illness, you should be able to return to your normal activities without any reason for concern. Your doctor will talk to you about what you can expect and any activity limitations depending on your age, health, activity level and the cause of your pericarditis.
Sometimes the attacks recur every few months and anti-inflammatory medications are needed for years to manage symptoms.
Appointments
Call toll-free 800.659.7822 to make an appointment.
Virtual Second Opinion
Cleveland Clinic's Second Opinion program connects patients to the expertise of top Cleveland Clinic specialists without the time and expense of travel. Through our secure web platform, patients can submit their detailed health information, medical records and diagnostic test results. The most appropriate Cleveland Clinic expert is assigned to the consultation and will render a detailed second opinion. The report includes commentary about the diagnosis and treatment options or alternatives and recommendations regarding future therapeutic considerations. Patients are also able to send additional questions to the physician who provided the report. Online medical second opinions are available for more than 1,200 medical diagnoses.
Talk to a Heart Nurse
For over 15 years Heart, Vascular & Thoracic resource nurses have been offering assistance to people who have questions or concerns about heart, vascular and thoracic conditions. Nurses are available to help with questions on symptoms, diagnoses, treatment options, Cleveland Clinic services and doctors, etc. The nurses are available weekdays from 8:30 a.m. – 4 p.m., Eastern Time, through phone or email. If you need help, you may contact a nurse.
Why Choose Us?
About Cleveland Clinic's Heart & Vascular & Thoracic Institute
The Sydell and Arnold Miller Family Heart, Vascular & Thoracic Institute at Cleveland Clinic is one of the largest cardiovascular specialty groups in the world, providing patients with expert medical and surgical care management and a full range of therapies. Cleveland Clinic is nationally ranked and globally recognized as the world leader in cardiovascular care.
Our areas of expertise combine research, education and clinical practice to provide innovative and scientifically-based treatments for cardiovascular disease. The commitment of our physicians and scientists to the prevention and cure of cardiovascular disease has led to innovative care, better outcomes and improved quality of life for patients with cardiovascular disease.
Glossary of Terms
Acute pericarditis: Inflammation of the pericardium that develops suddenly and is accompanied by the sudden onset of symptoms.
Cardiac tamponade: A severe compression of the heart that impairs its ability to function. Cardiac tamponade is a medical emergency that requires prompt diagnosis and treatment.
Chronic pericarditis: Inflammation of the pericardium that lasts for three months or longer after the initial acute attack.
Constrictive pericarditis: A severe form of pericarditis in which the inflamed layers of the pericardium stiffen, develop scar tissue, thicken and stick together. Constrictive pericarditis interferes with the normal function of the heart.
Infectious pericarditis: Pericarditis that develops as the result of a viral, bacterial, fungal or parasitic infection.
Idiopathic pericarditis: Pericarditis that does not have a known cause.
Incessant pericarditis: Pericarditis with symptoms that persist for 3 months.
Interleukin receptor antagonists (IL-1RN): A protein that binds to interleukin-1 receptors, a drug with anti-rheumatic properties.
Pericardium: The thin, two-layered, fluid-filled sac that covers the outer surface of the heart.
Pericardial effusion: Excess fluid build-up in the pericardium.
Pericardial window: A minimally invasive surgical procedure performed to drain fluid that has accumulated in the pericardium. This surgical procedure involves a small chest incision through which an opening is made in the pericardium.
Pericardiectomy: Surgical treatment of pericarditis that involves the removal of a portion of the pericardium.
Pericardiocentesis: A procedure performed to drain excess fluid from the pericardium with a catheter.
Recurrent pericarditis: Pericarditis with symptoms that improve for 4-6 weeks and then recur.
Traumatic pericarditis: Pericarditis that develops as the result of injury to the chest, such as after a car accident.
Uremic pericarditis: Pericarditis that develops as the result of kidney failure.
Resources
Center for the Diagnosis and Treatment of Pericardial Diseases
The multi-disciplinary team of experts in the Center for the Diagnosis and Treatment of Pericardial Diseases includes cardiologists, cardiac surgeons, nurses and other specialists, such as rheumatologists and infectious disease physicians. We provide:
- A thorough evaluation of patients using state-of-the-art diagnostic testing
- Multi-disciplinary approach to comprehensive care for patients with pericardial diseases
- Ongoing research and education to provide patients with high-quality and innovative therapies
Learn More
- Learn more about pericarditis by visiting Cleveland Clinic’s Heart, Vascular & Thoracic Institute website
- Watch videos on pericardial diseases and treatments presented by Cleveland Clinic specialists
- Sign up for our e-newsletter, and get tips on maintaining a heart healthy lifestyle, recipes and essential health news
- Listen to podcasts from our Cleveland Clinic Heart, Vascular & Thoracic physicians.
