People with premenstrual dysphoric disorder (PMDD) have PMS symptoms (bloating, headaches and breast tenderness) in the weeks before their period. But PMDD also causes severe anxiety, depression and mood changes. Some people with PMDD become suicidal. Hormonal birth control and antidepressants can relieve symptoms.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
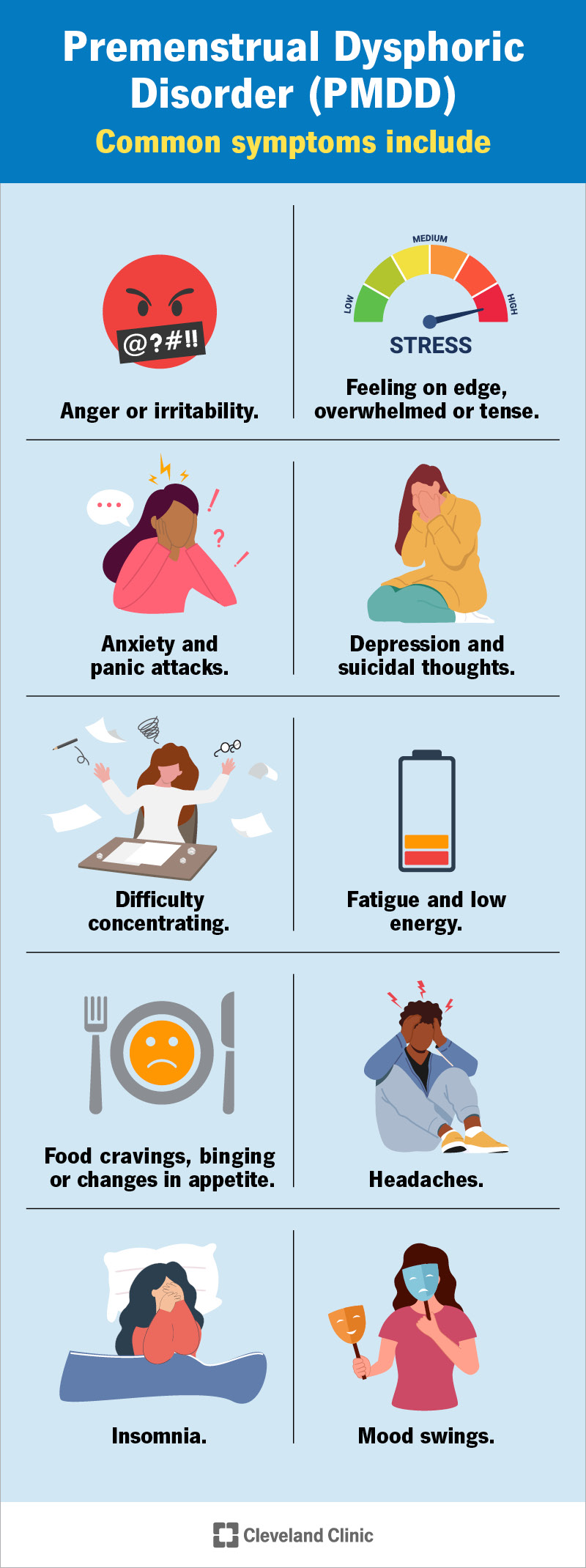
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/9132-premenstrual-dysphoric-disorder-pmdd)
Premenstrual dysphoric disorder (PMDD) is a more serious form of premenstrual syndrome (PMS). It causes physical and emotional symptoms every menstrual cycle in the week or two before your period. PMS causes bloating, headaches and breast tenderness.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
With PMDD, you might have PMS symptoms along with extreme irritability, anxiety or depression. These symptoms improve within a few days after your period starts, but they can be severe enough to interfere with your life.
PMDD affects up to 10% of people who have periods.
Symptoms of PMDD vary by individual. They tend to appear a week or two before menstruation and go away within a few days of your period starting. In addition to PMS symptoms like cramping and bloating, you may have:
For some people, symptoms of PMDD last until menopause.
Experts don’t know why some people get PMDD. Decreasing levels of estrogen and progesterone hormones after ovulation and before menstruation may trigger symptoms. Serotonin, a brain chemical that regulates mood, hunger and sleep, may also play a role. Serotonin levels, like hormone levels, change throughout your menstrual cycle.
You may be more prone to PMDD if you have:
Advertisement
Untreated PMDD can lead to depression and, in severe cases, suicide. The disorder can cause severe emotional distress and negatively affect relationships and careers.
If you’re experiencing suicidal thoughts and live in the U.S., call or text the Suicide and Crisis Lifeline at 988. This national network of local crisis centers provides 24/7 free and confidential support. You can also dial 988 if you’re worried about a loved one who may need help.
Your healthcare provider will take a medical history and evaluate your symptoms. You may need to track your symptoms through one or two menstrual cycles. To diagnose PMDD, your provider will look for five or more PMDD symptoms, including one mood-related symptom. Your provider will rule out or diagnose other conditions such as anxiety, depression or reproductive disorders.
Your healthcare provider may recommend one or more of these treatments to help manage PMDD:
There are some ways to manage symptoms of PMDD that don’t involve medication. For example, you can practice yoga, try meditation or find other ways to improve your mood. Changing certain aspects of your diet may also bring relief. Additionally, support groups or resources may help you. Be sure to talk to your provider about all the treatment options available.
With treatment, most people with PMDD get relief from their symptoms and are able to enjoy life more fully. Talking to a mental health specialist or joining a support group may also help. Most people don’t have symptoms after menopause.
Treating existing depression or anxiety may make it less likely that PMS could become PMDD. But PMDD could be related to the way your hormones work, and you might not be able to prevent it. In that case, treatment can bring relief.
You should call your healthcare provider if you experience:
If you have PMDD, you may want to ask your healthcare provider:
Advertisement
PMDD and PMS are similar in that they both happen in the week or two before your period begins when your hormone levels drop. They both cause physical symptoms like cramps, headaches or bloating. However, PMDD also causes serious symptoms that may disrupt your mood.
Symptoms of PMDD start 10 to 14 days before your period and usually go away within the first two days of your period. This means that a person with PMDD could feel the effects of PMDD for over two weeks each menstrual cycle. During this time, it’s important to follow your provider’s recommendations for treatment. Take extra care of yourself and lean on loved ones for support.
PMDD is a mental health condition listed in the DSM-5 as a "depressive disorder." The DSM-5 stands for Diagnostic and Statistical Manual of Mental Disorders and is a criteria for diagnosing mental health conditions.
No. PMDD and bipolar disorder aren’t the same condition. They do, however, have similar symptoms. During a depressive episode in bipolar disorder, you may feel irritable or like you’re losing control. You may also have suicidal thoughts. It’s important to get support and seek help if you have symptoms of either condition.
PMDD is a serious disorder that can negatively affect your life, relationships and career. You may harm themselves or others. If you consistently experience severe depression and anxiety or other PMDD symptoms in the weeks leading up to your period, seek help from your healthcare provider. Medications can get hormone or serotonin levels in check so that you feel more like yourself. PMDD isn’t a problem you have to live with. Don’t put off getting the medical and mental health care you need.
Advertisement


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
From routine pelvic exams to high-risk pregnancies, Cleveland Clinic’s Ob/Gyns are here for you at any point in life.
