Cerebral palsy (CP) is a group of neurological conditions that affect muscle movement, posture and coordination. A brain injury or abnormal development causes it before, during or shortly after birth. While there’s no cure, early treatment may help improve comfort, mobility and daily life.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
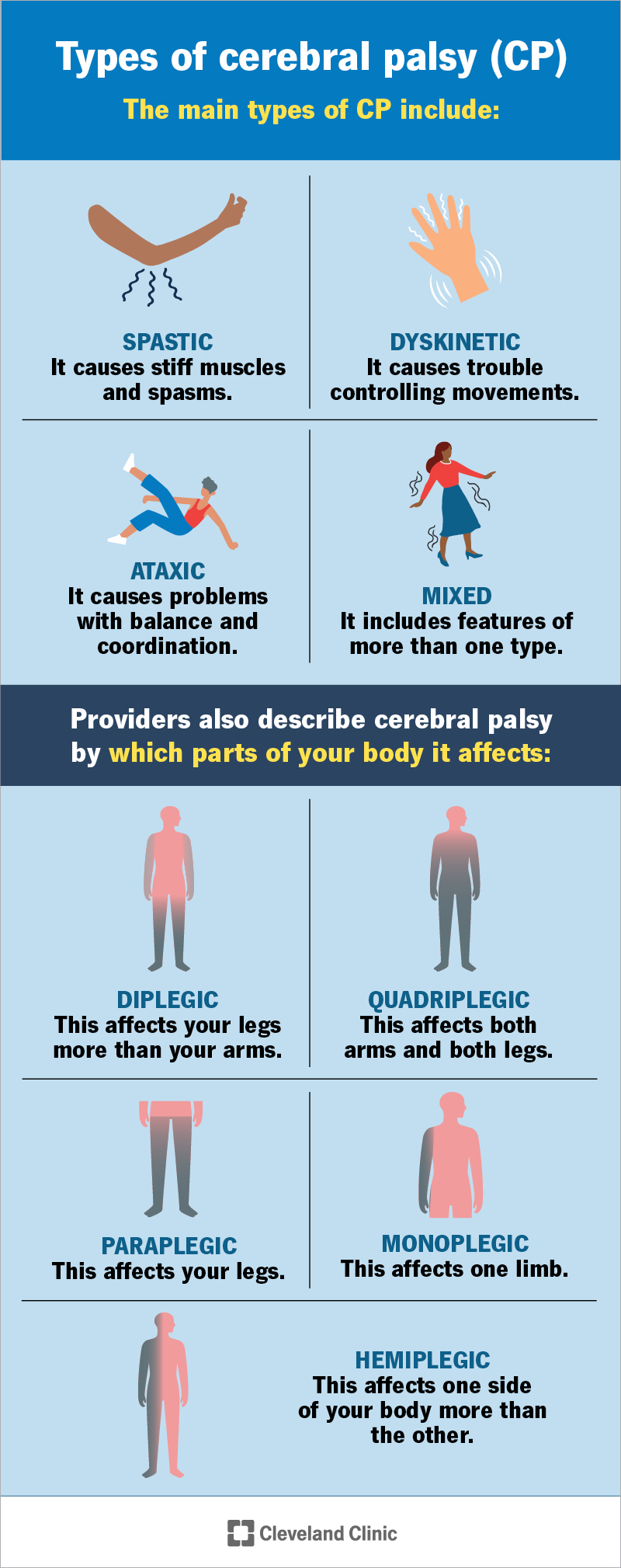
Image content: This image is available to view online.
View image online (https://my.clevelandclinic.org/-/scassets/images/org/health/articles/cerebral-palsy)
Cerebral palsy (CP) is a group of neurologic conditions that happens when your brain doesn’t develop as expected or gets injured before, during or soon after birth.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
CP affects movement, posture and coordination. It may cause permanent disabilities.
While the brain injury doesn’t worsen over time, symptoms and physical challenges may change as your child grows.
CP affects about 3 out of every 1,000 children in the United States. There’s no cure for CP. But treatment focuses on managing symptoms and improving daily life, comfort and independence. Your care team will work with you to create a plan that fits your needs.
The main types of CP include:
Providers also describe CP by which parts of your body it affects:
Symptoms may affect how your child moves, feels and interacts with the world. Symptoms that affect their muscles could include:
Advertisement
The following are experiences that your child or a caregiver may report since it can be hard for a child to vocalize what they’re feeling:
CP can look different for each person. A parent, caregiver or provider might notice the following signs:
Cerebral palsy happens when your baby’s brain doesn’t develop as expected or experiences damage. The damage can happen before birth, during birth or shortly after birth.
Sometimes, providers can identify the exact cause. Other times, they can’t find a clear reason. Your child’s provider can explain what may have happened in your child’s case.
These happen during fetal development:
These happen around the time of delivery:
These happen in the first months or years of life:
CP isn’t usually a genetic condition. Most cases happen because of abnormal brain development or a brain injury before, during or shortly after birth.
But genetics can play a role in some cases. Chromosomal abnormalities or genetic susceptibility (a higher chance of developing a condition because of your genes) may contribute. Providers may recommend genetic testing if your child has specific physical features, brain malformations or a biological family history.
Certain factors may increase your baby’s risk of developing this condition. These include:
Certain conditions during pregnancy may increase the risk, such as:
Having one or more risk factors doesn’t mean your child will develop CP, but it might increase the chance. Your provider can explain your child’s specific risks and what they mean.
Advertisement
This condition can lead to complications over time, including:
As your child gets older, this condition may also weigh on their mental health. They may develop symptoms of depression and anxiety. Seeing a mental health provider, like a therapist or counselor, may help them cope.
Healthcare providers diagnose this condition by reviewing your child’s medical history and doing a detailed physical exam. They’ll ask about pregnancy and birth history, developmental milestones, like sitting or walking, and any known biological family history or risk factors.
Providers often order a brain MRI. These imaging tests create detailed pictures of your child’s brain. It can show areas of abnormal development or injury. In newborns, providers may use a cranial ultrasound to look for bleeding or certain types of brain damage.
Your child’s provider can tell you what tests they recommend and why they are necessary.
A diagnosis usually happens between 1 and 2 years of age. Sometimes, it happens sooner if your child has a high-risk case.
Advertisement
There isn’t a cure for cerebral palsy, but treatment may help your child move better and stay comfortable. Your child’s care team will set realistic goals and adjust them over time.
Common treatments include:
Your child’s treatment plan will depend on their specific symptoms, strengths and goals. Your care team will guide you through each step.
Your child’s provider might recommend medicines based on their specific needs. Some options might include:
Advertisement
In moderate to severe cases, your child may need surgery. Options could include:
Call your child’s provider right away if you notice:
CP is a permanent, lifelong condition that affects each child differently. Your child’s outlook mostly depends on the type, how quickly they gain motor skills and their thinking abilities.
Motor development, especially walking, is an important part of their prognosis. Studies show that many children who walk on their own do so by age 3. Children who walk with support may reach that milestone by age 9. If your child isn’t walking by age 9, they’re unlikely to walk even with support.
If your child is able to walk, they may do so with or without support. Support may look like crutches, a walker or a cane. Some people use a wheelchair for mobility.
Walking ability varies widely. Some may be able to walk short distances but use a wheelchair for longer distances or when they feel tired. Your provider can help you understand what to expect based on the type and severity.
Many people with this condition live into adulthood. Life expectancy depends on how severe the condition is and whether your child has other serious health issues.
Breathing problems, like aspiration pneumonia (a lung infection caused by food or liquid going into your lungs), are common health concerns in severe cases.
Your care team can help you understand what to expect based on your child’s specific health needs.
You can’t always prevent this condition. Many cases happen for reasons that are out of your control. If you’re wondering whether something could have been done differently, those feelings are understandable.
Some steps may help lower the risk:
Even when families do everything right, CP can still happen. What matters most is early support and care to help your child thrive.
Cerebral palsy (CP) doesn’t have a one-size-fits-all treatment plan. What your child experiences can be very different from that of another. What matters most is getting the support your child needs to help them stay comfortable, healthy and independent.
Your care team will work with you to understand your child’s needs, answer questions and adjust treatment as they grow. It’s about more than just managing symptoms — it’s about helping your child live the fullest life possible, in a way that works for them.


Sign up for our Health Essentials emails for expert guidance on nutrition, fitness, sleep, skin care and more.
Learn more about the Health Library and our editorial process.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
Cleveland Clinic’s health articles are based on evidence-backed information and review by medical professionals to ensure accuracy, reliability and up-to-date clinical standards.
If you have a neurological condition, you want expert advice. At Cleveland Clinic, we’ll work to create a treatment plan that’s right for you.
